
Parasitology — MCQs

On this page
Which worm causes myocarditis?
In a patient presented with a fever and a positive filarial antigen test, what is the next appropriate method of management?
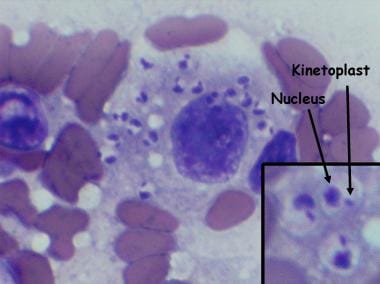
A lady from West Rajasthan presented with an ulcer surrounded by erythema on the right leg. Microscopy of the biopsy from the edge of the ulcer showed organisms with dark staining nuclei and kinetoplast. What is the most likely causative agent? (Refer to the provided image)
A boy presented with a fever and chills. Rapid test was positive for specific antigen HRP-2. Which of the following species of Plasmodium is the most likely causative agent?
Identify the parasite shown in the image.

Sheathed microfilariae with two nuclei at the tail tip is suggestive of?
Green frothy vaginal discharge is produced by –
A 15-year-old boy presented with fever and chills for 3 days. On examination, he was found to have delayed skin pinch time and dry oral mucosa. A peripheral blood smear revealed multiple delicate ring forms within red blood cells, with some red blood cells containing more than one ring form. No other developmental stages were observed. Identify the pathogen involved.
Sabin-Feldman dye test is used for diagnosis of which of the following conditions:
Cutaneous larva migrans is caused by which organism?
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app