
Parasitology — MCQs

On this page
A 40-year-old man presents with muscle pain, fever, and difficulty breathing. He reports having eaten undercooked pork recently. Muscle biopsy shows encysted larvae. What is the most likely organism?
A 6-year-old child presents with severe diarrhea and dehydration. Stool examination reveals the presence of trophozoites with characteristic 'falling leaf' motility. What is the most likely causative agent?
Which parasite is the most common cause of chronic malabsorptive diarrhea worldwide and is characterized by pear-shaped trophozoites?
A 45-year-old female presents with abdominal pain, jaundice, and fever. An abdominal CT scan reveals multiple liver abscesses, and aspiration yields anchovy paste-like pus. What is the most likely etiological agent responsible for these findings?
An immunocompromised patient presents with diarrhea, abdominal pain, and weight loss. Stool microscopy reveals acid-fast oocysts. Evaluate the diagnostic results to identify the most likely causative agent.
Which stool examination technique is considered the most effective for detecting Giardia lamblia based on diagnostic sensitivity and specificity?
Which organism is most commonly involved in the pathogenesis of diarrhea in HIV-infected patients and is diagnosed by modified acid-fast staining of fecal matter?
A 28-year-old man presents with fever and lymphadenopathy. A blood smear shows trypomastigotes with an undulating membrane. Which disease is most likely?
A 30-year-old female presents with abdominal pain, diarrhea, and weight loss. Stool microscopy reveals ova with a characteristic lateral spine. What is the most likely diagnosis?
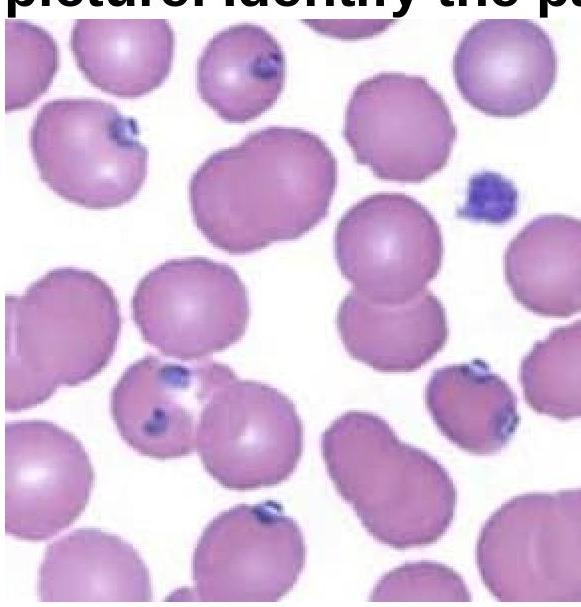
A 15-year-old boy presented with fever and chills for 3 days. On examination, he was found to have delayed skin pinch time and dry oral mucosa. Identify the pathogen involved based on the provided peripheral blood smear image.
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app