
Parasitology — MCQs

On this page
What is the primary causative agent of scabies?
A 23-year-old male returns from a hiking trip with complaints of diarrhea, abdominal cramps, and fatigue. Stool microscopy reveals flagellated trophozoites. What is the most likely diagnosis?
A patient with AIDS presents with fever and weight loss. A biopsy of a lymph node shows intracellular amastigotes. Which organism is likely responsible?
A patient develops watery diarrhea after attending a wedding. Stool examination reveals acid-fast oocysts. Which organism is most likely responsible?
A neonate develops severe jaundice and hepatosplenomegaly shortly after birth. Laboratory tests reveal elevated IgM antibodies against Toxoplasma gondii. What is the most likely route of transmission?
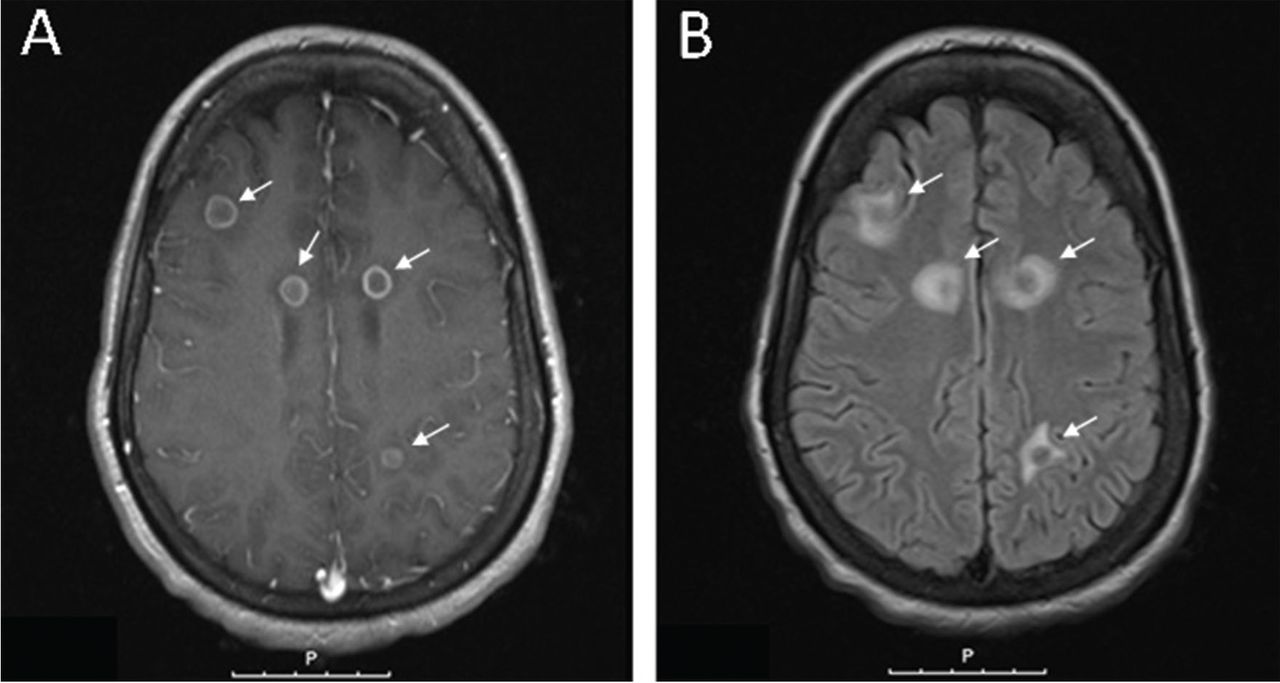
In an HIV-positive patient presenting with headache, confusion, and fever, which of the following is the most likely causative organism for the multiple ring-enhancing lesions observed on MRI?
A 40-year-old man who recently traveled to South America presents with a chronic, ulcerative lesion on his arm. A biopsy reveals amastigotes within macrophages. What is the most likely diagnosis?
A patient presents with diarrhea, bloating, and weight loss. Stool analysis shows pear-shaped, flagellated protozoa. What is the most likely diagnosis?
A 45-year-old male presents with diarrhea and abdominal pain after consuming undercooked beef. Stool examination reveals eggs. What is the most likely cause?
Which pathogen is commonly responsible for causing diarrhea in patients with HIV/AIDS?
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app