
Parasitology — MCQs

On this page
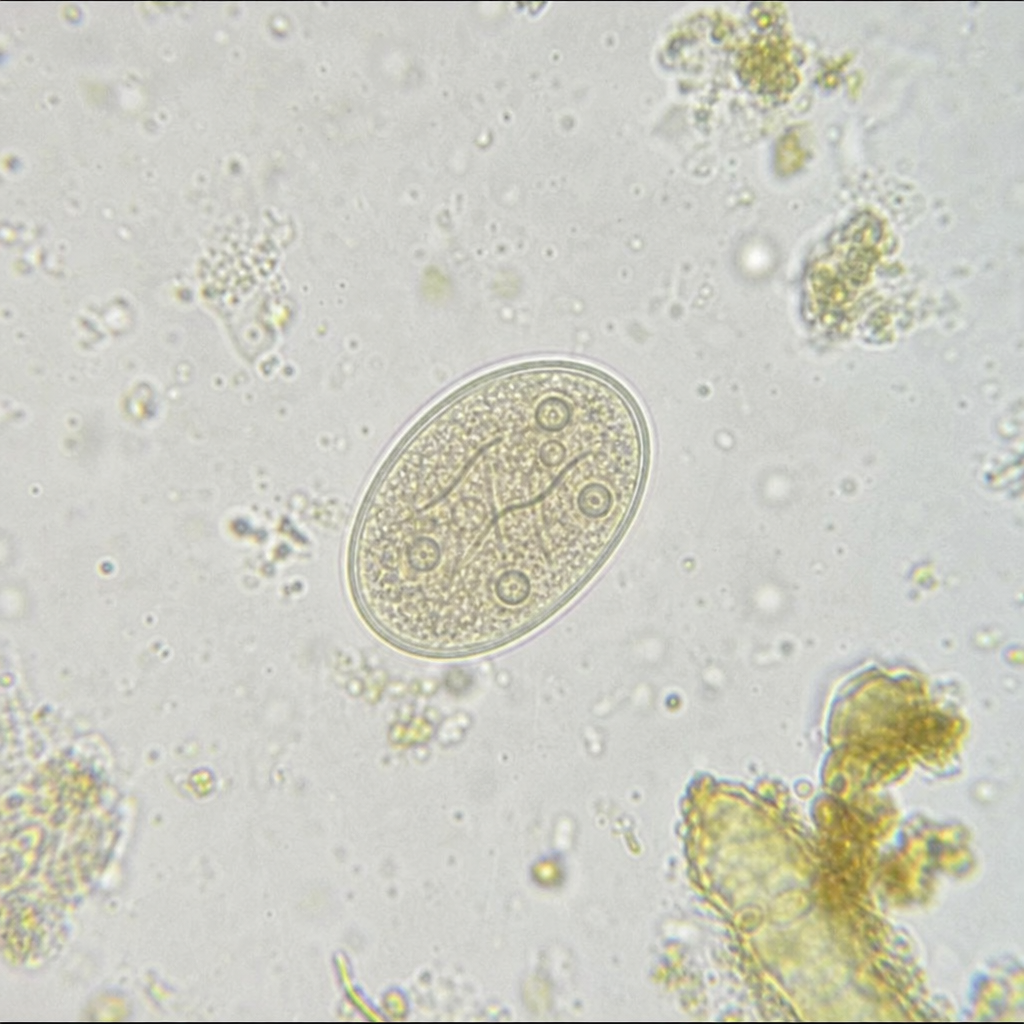
Based on the microscopic image showing an oval cyst containing 4 nuclei with visible fibrils under stool microscopy examination, identify the parasitic organism:
A known HIV patient on anti-retroviral therapy presented with diarrhea of six months duration. Stool microscopy showed 10-30 micrometer cysts, Kinyoun stain was positive. What is the most likely diagnosis?
Episodes of repeated thin stools with mucus, subjective feeling of fever and lower abdominal pain, with leukocytes in stool. Which of the following is likely?
A wet mount of vaginal discharge shows motile, flagellated protozoa. Which organism is most likely causing this infection?
A blood smear from a patient with cyclic fevers shows Maltese cross formations within red blood cells. Which organism is the likely cause?
A 30-year-old man with HIV presents with chronic diarrhea. Stool examination reveals small, spherical, acid-fast oocysts. What is the causative agent?
Which is the primary host cell for Plasmodium vivax during its human life cycle?
Assertion: Plasmodium falciparum does not show the schizont stage in the peripheral blood. Reason: This is due to cytoadherence of infected RBCs to the vascular endothelium.
Which of the following organisms show parthenogenesis?
What is the best investigation for identifying malaria species?
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app