
Parasitology — MCQs

On this page
The life cycle of filaria in the mosquito is described as:
Cyclodevelopmental life cycle is seen in:
All of the following are helminthic waterborne disease except?
A man on return from East Asia complains of pain in abdomen, jaundice, with increased alkaline phosphatase and conjugated hyperbilirubinemia. Ultrasound shows blockage in the biliary tree. What could be the cause?
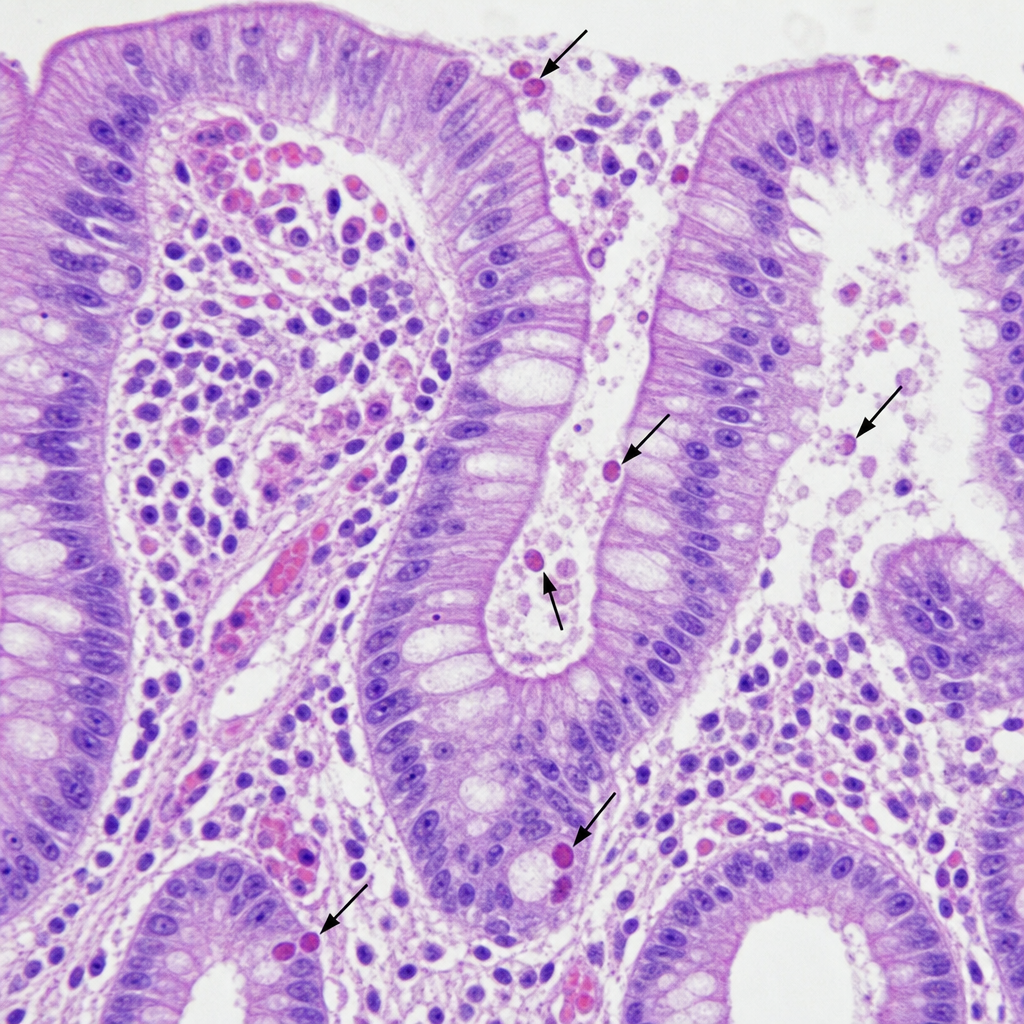
A 35-year-old heterosexual patient diagnosed with HIV presents with watery diarrhea. The colonoscopic biopsy is shown below. Which of the following is your most probable diagnosis?
Reduvid bug transmits-
Chagas disease is transmitted by the following:
Reduviid bug is a vector for the transmission of:
Chiggerosis is due to
What type of life cycle does the malaria parasite exhibit?
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app