
Parasitology — MCQs

On this page
Casoni's test is used in the diagnosis of which of the following infections?
Which micro–organism is responsible for classical presentation of hydrocephalus, chorioretinitis, intracerebral calcification ?
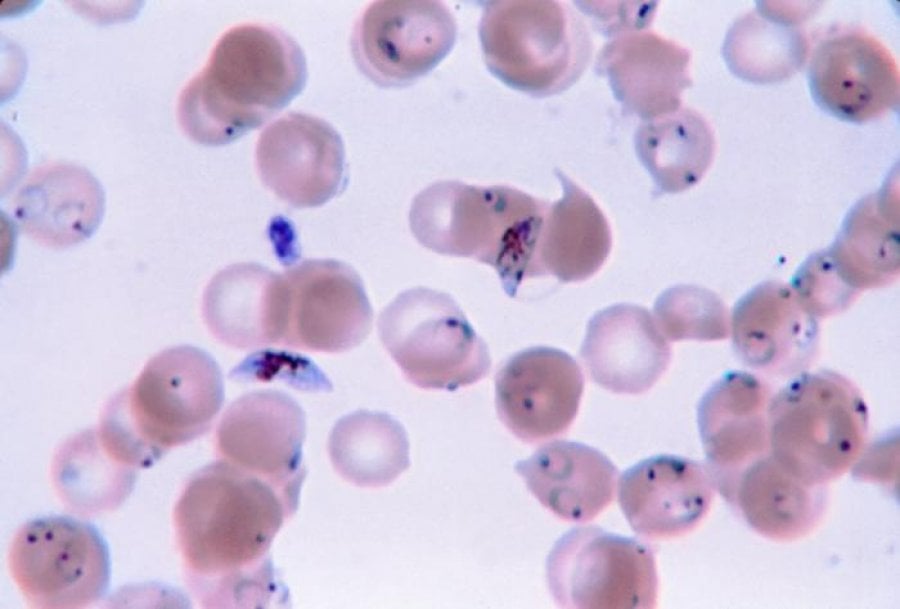
A 24-year-old patient presents with a high-grade fever, headache, and weakness since 5 days. He gives a history of blood transfusion 4 months back. The microscopic examination of the thin blood smear is given below. What is the most probable causative agent?
Sabin Feldman dye test is used for:
Infection caused by which of the following organism may mimic as malignancy?
An Egyptian fisherman develops lower abdominal pain and pain on urination, and reports seeing blood in his urine. Which of the following parasites is the most likely cause of urinary symptoms in this patient?
Which of the following is the most common central nervous system parasitic infestation-
Painless terminal hematuria is seen as one of the manifestations in the infection caused by ?
Peripheral blood smear in Plasmodium falciparum infection may show all of the following except -
Man is the only host for
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app