
Parasitology — MCQs

On this page
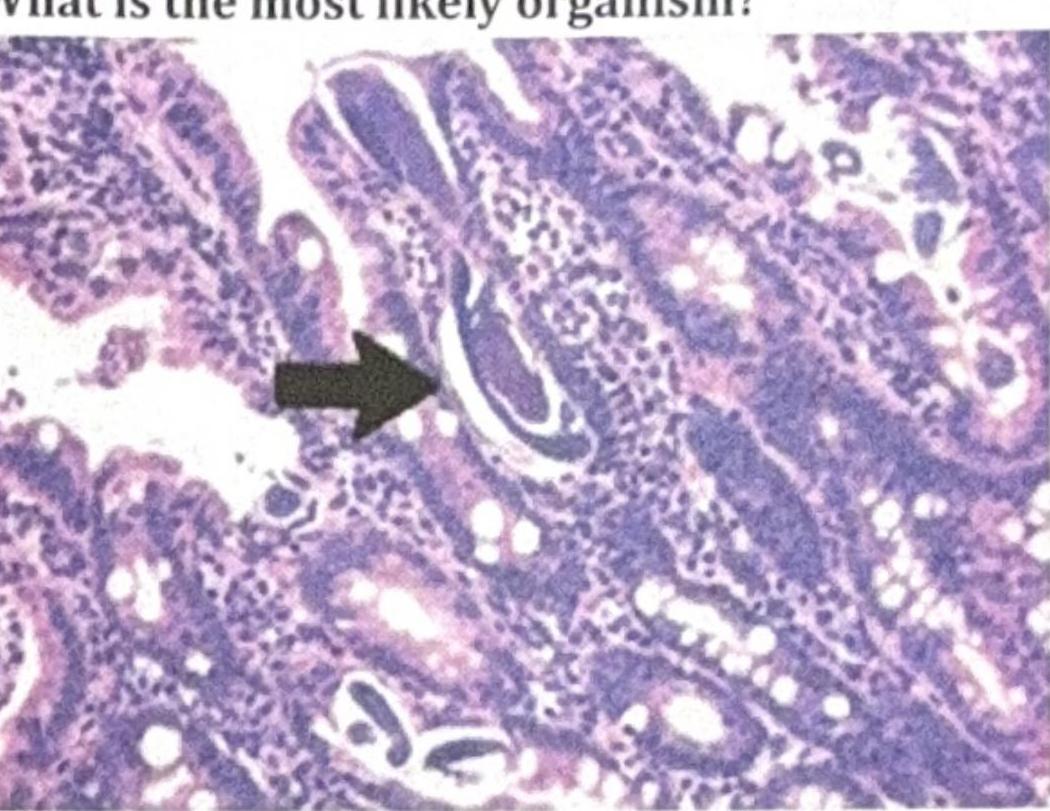
A patient on steroids presented with nocturnal cough and chronic urticaria. An intestinal biopsy was done, and the organism shown in the image was identified. What is the most likely organism?
Name the parasite whose microfilariae have a sheath and no nuclei at the tail end.
On Ziehl-Neelsen (ZN) staining oocysts of size 8-10 µm are visible. Identify the organism.
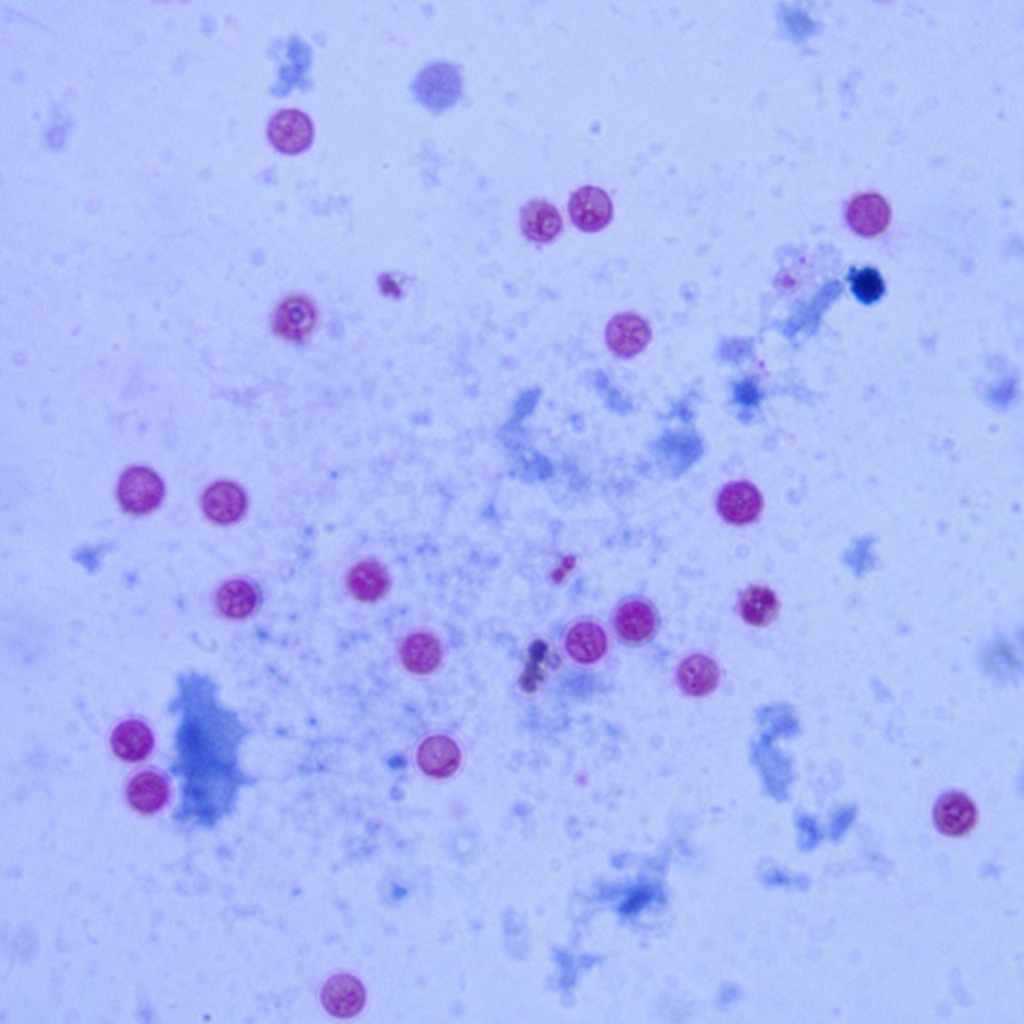
An HIV patient came to the clinic with a history of diarrhea. Stool microscopy showed the oocysts that were 4-6 µm in size. The image is shown below. Identify the organism.
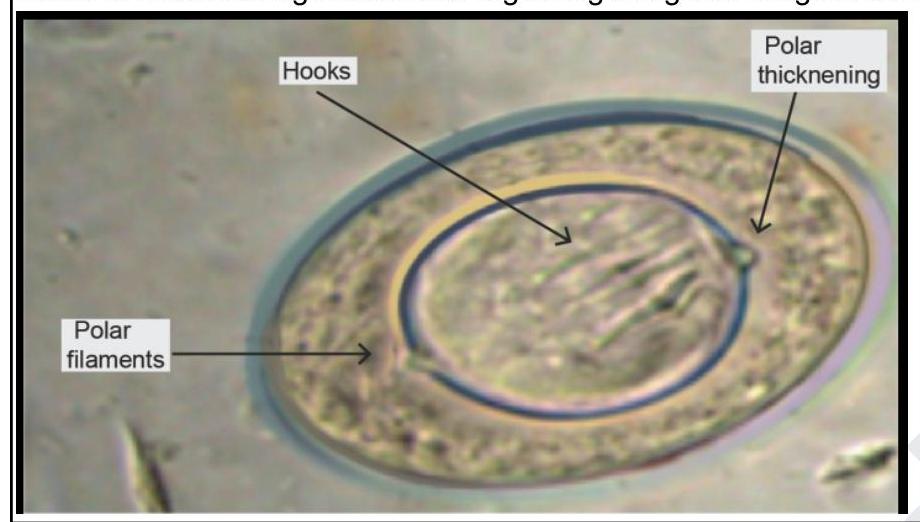
Which of the following statements regarding the given image is correct?
A person handling cat feces is at risk of transmitting an infection. Which of the following is the infective stage of the organism transmitted through cat feces?
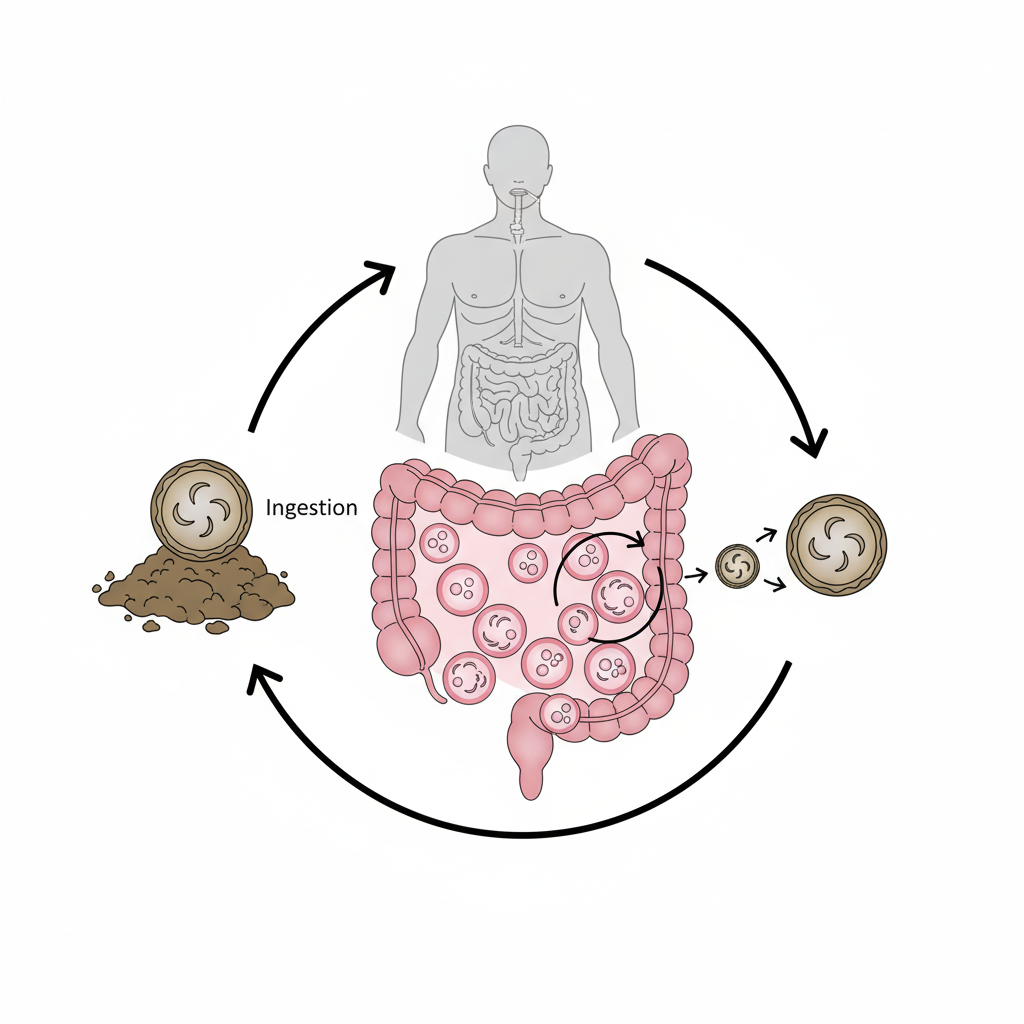
Identify the organism from the life cycle shown in the image given below
A parasitic smear shows 'copper penny' appearance of RBCs. Which morphological feature would confirm Plasmodium falciparum?
A parasitic smear shows 'double dot' chromatin pattern. Which morphological feature would confirm Babesia infection?
Most sensitive test for detecting microfilariae?
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app