
Parasitology — MCQs

On this page
Which one of the following statements is correct in the diagnosis of Giardiasis?
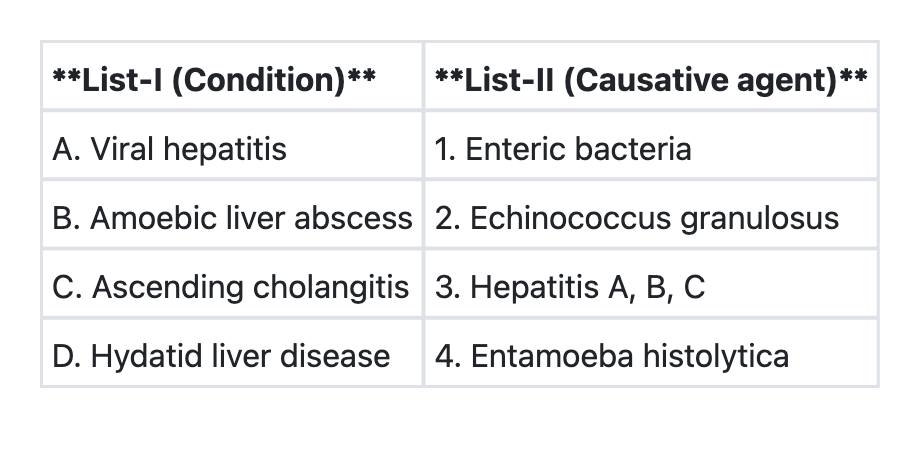
Match List-I with List-II and select the correct answer using the code given below the Lists:
Which of the following statements is true about hydatid disease?
A female presents with dysuria and vaginal discharge. Wet mount examination shows pear-shaped organisms. What is the most likely diagnosis?
Which of the following is TRUE about screening for Trichomonas vaginalis?
How does trichomoniasis affect HIV transmission?
A young boy who used to wash his contact lenses in tap water or with unhygienic lens fluid developed keratitis. Microscopy revealed an organism with spiked or star-shaped structures. Identify the correct organism responsible.
A woman presents with a chronic history of fever and lower limb swelling. The microscopic image of a parasite in her blood smear is shown. Identify the pathogen responsible for her condition.

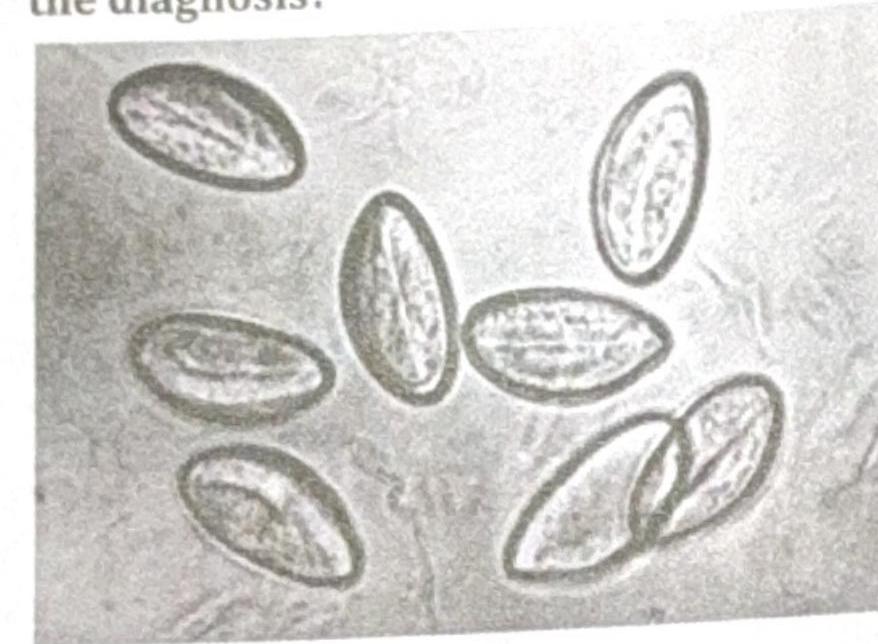
A child presented with perianal itching. The swab specimen is shown in the image. What is the diagnosis?
What is the vector for Leishmania, a parasite characterized by a prominent kinetoplast in its morphological forms?
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app