
Parasitology — MCQs

On this page
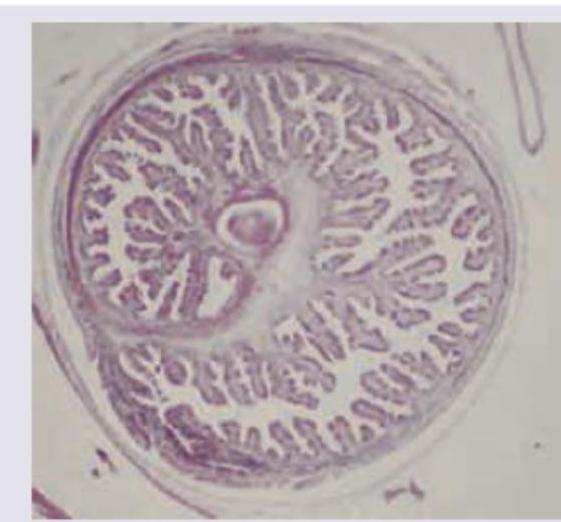
Which of the following parasite is shown below?
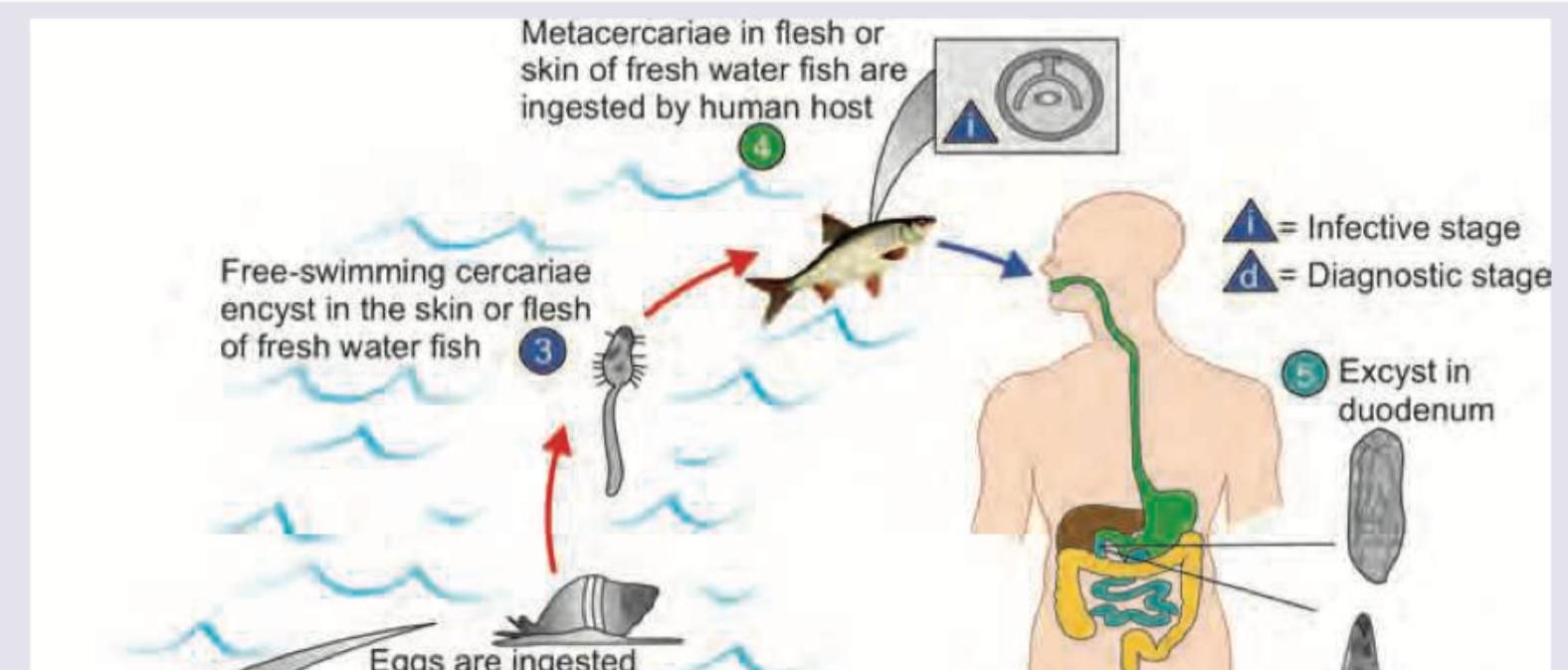
Which of the following life cycle is shown below?
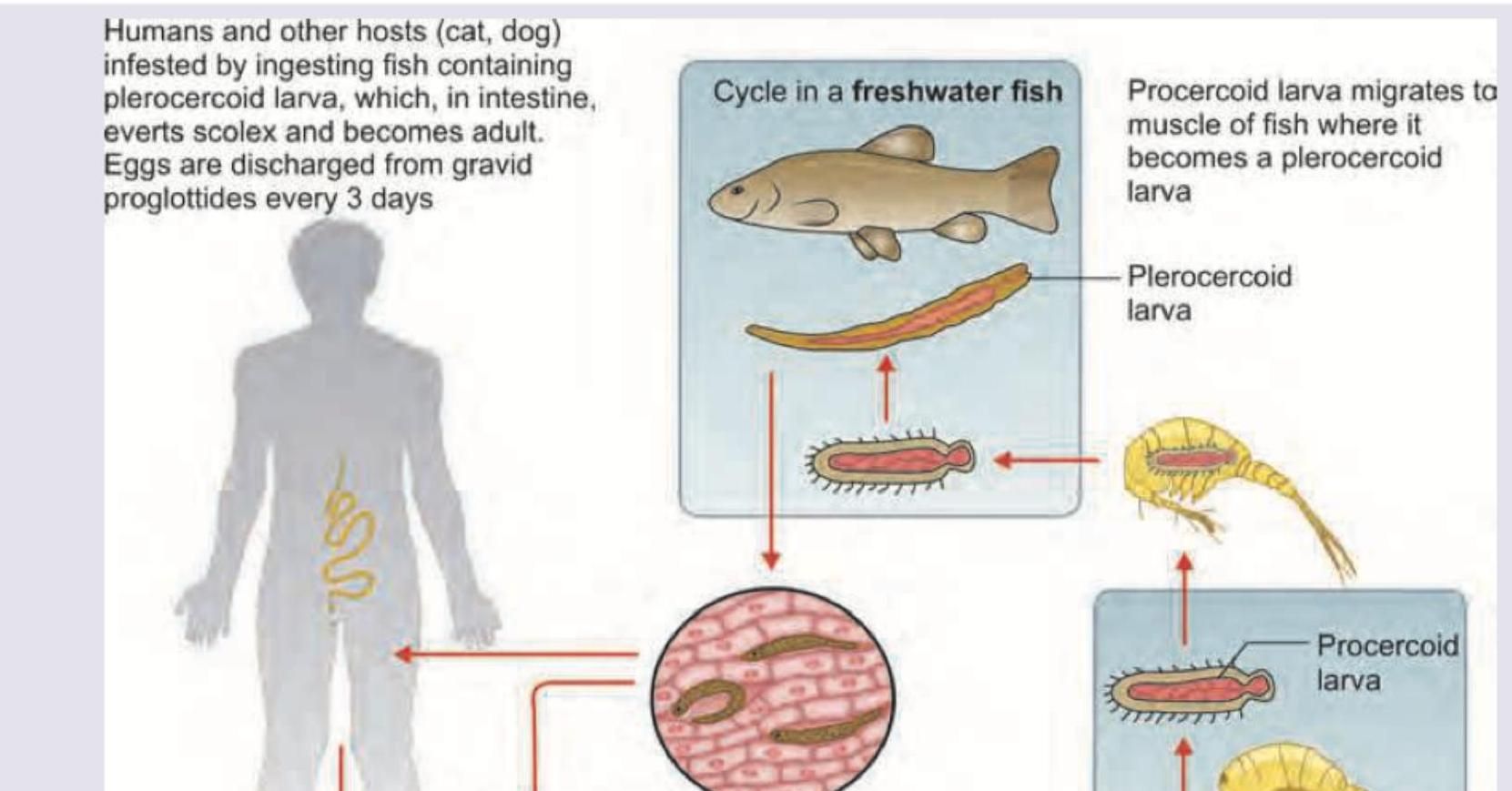
Which of the following life cycle is shown below?
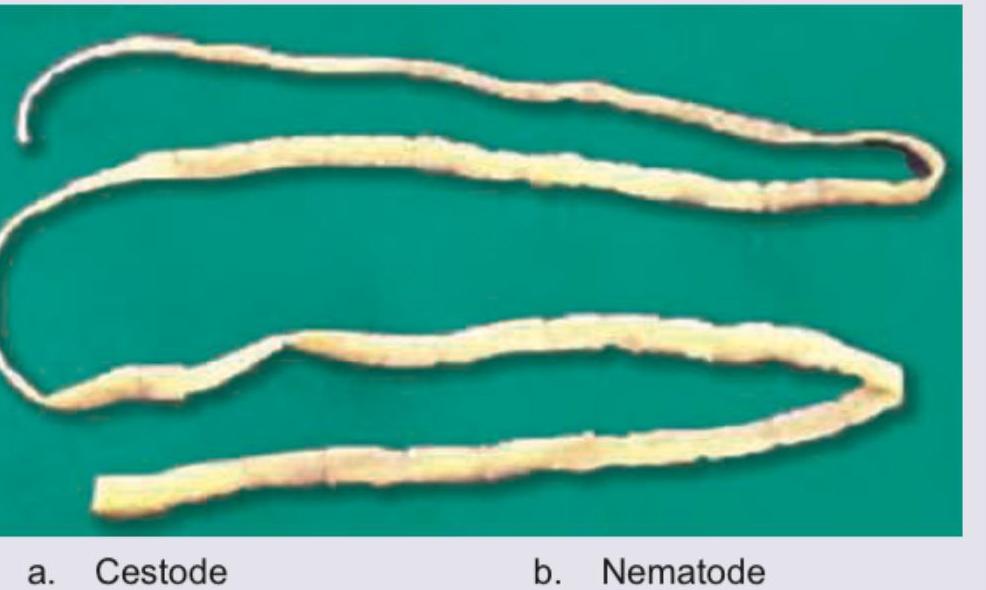
The following organism is called:
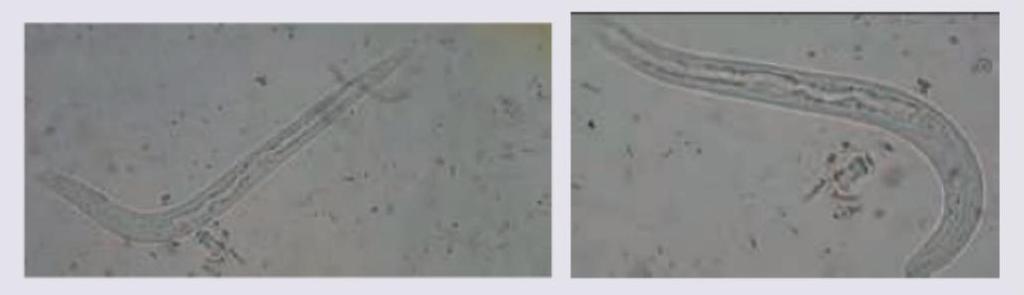
Post kidney transplantation, a patient presents with diarrhoea. The morphology of the worms is shown in the figure. Correct statement about the organism is: (AIIMS Nov 2018)
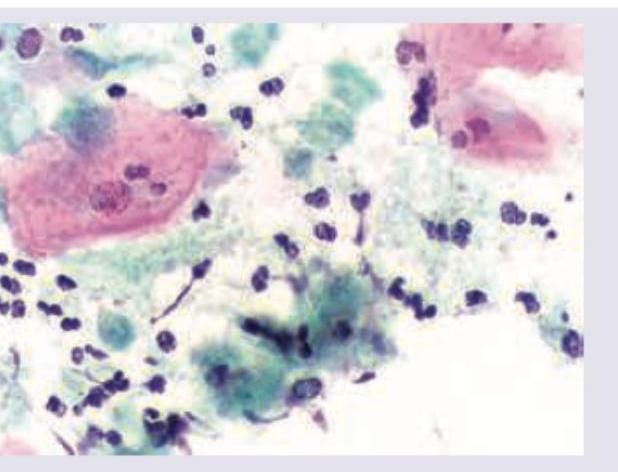
A stained smear of vaginal discharge shows the following. Identify the organism responsible.
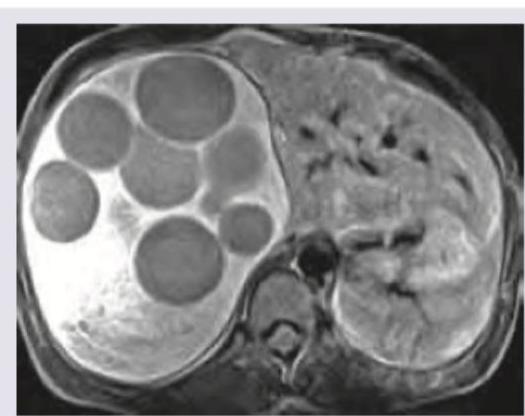
A 25 -year-old complains of a gradually enlarging painless mass in the right upper quadrant. Which among the following statement regarding this patient is false? (Recent NEET Pattern 2016-17)
Identify the parasite shown in the image.

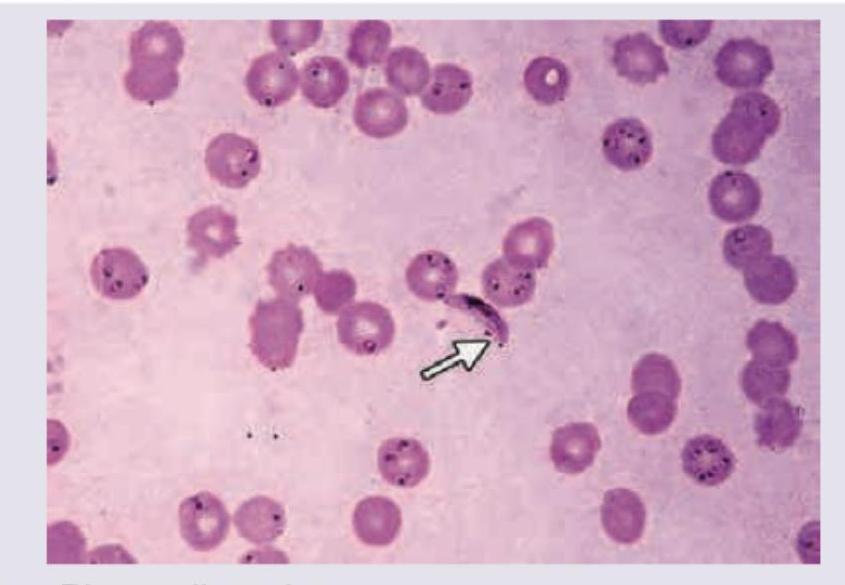
A 34-year-old lady presents with high-grade fever with chills and rigors. On examination, a firm spleen is felt 3 cm below costal margin. Peripheral smear was prepared. Diagnosis is:
Which one among the following vectors transmits the filaria *Loa loa*?
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app