
Parasitology — MCQs

On this page
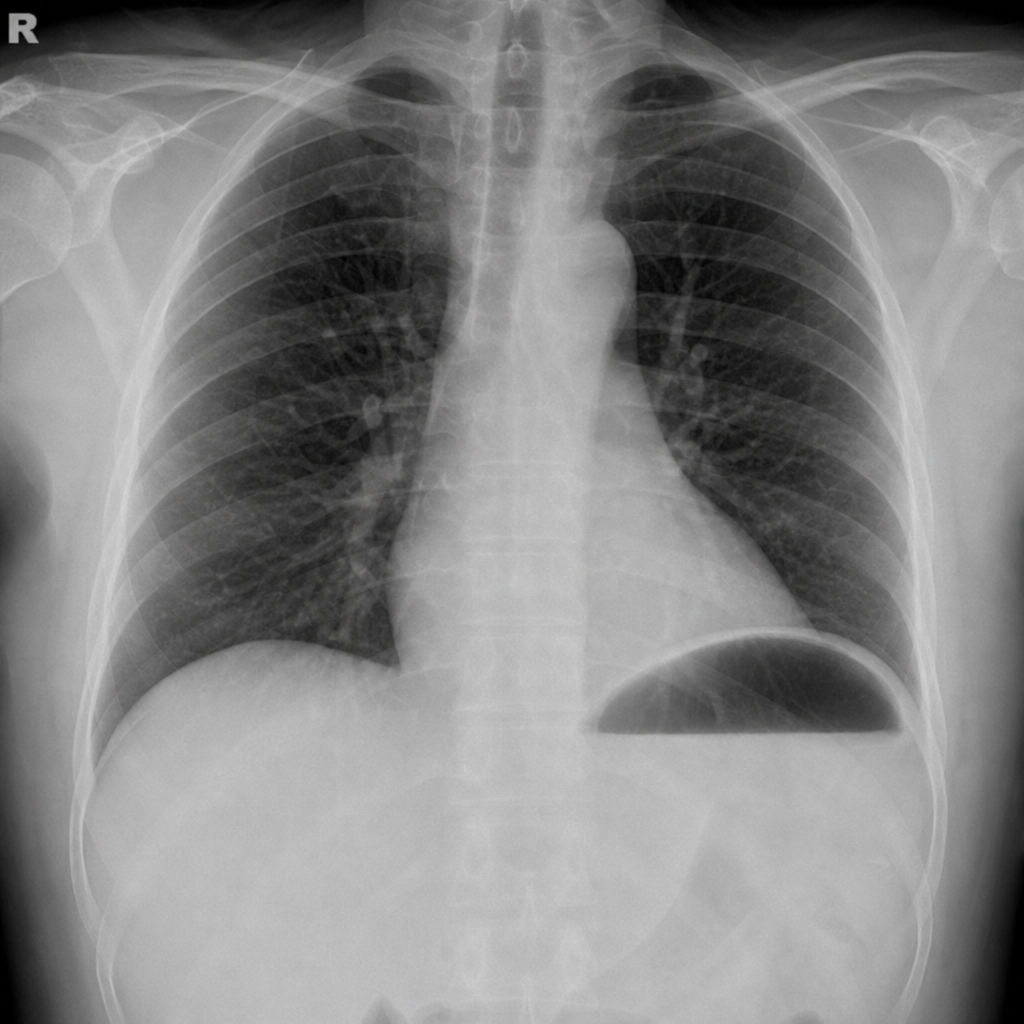
Which of the following is shown here?
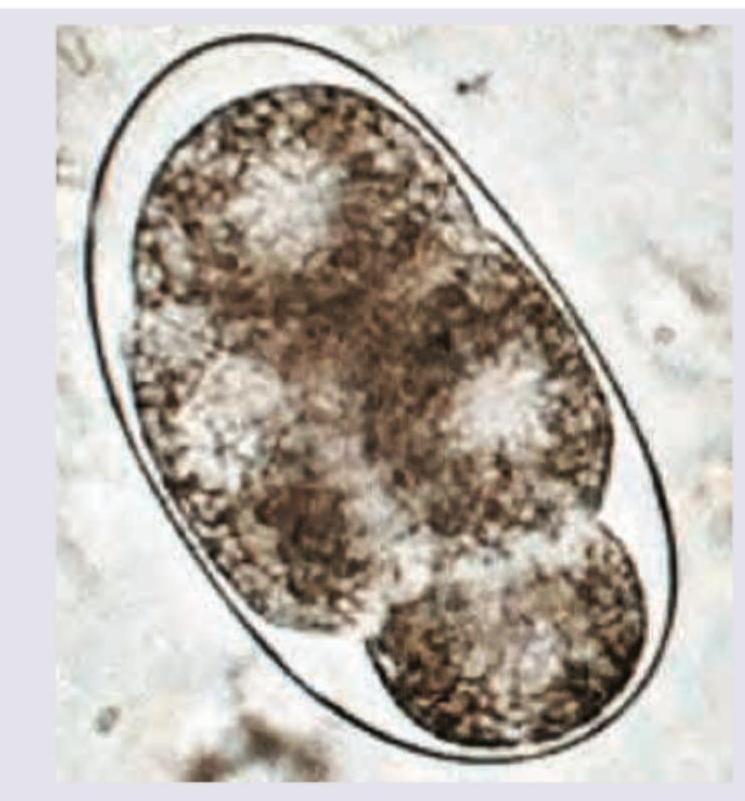
The image shown below shows egg of? (AIIMS May 2017)
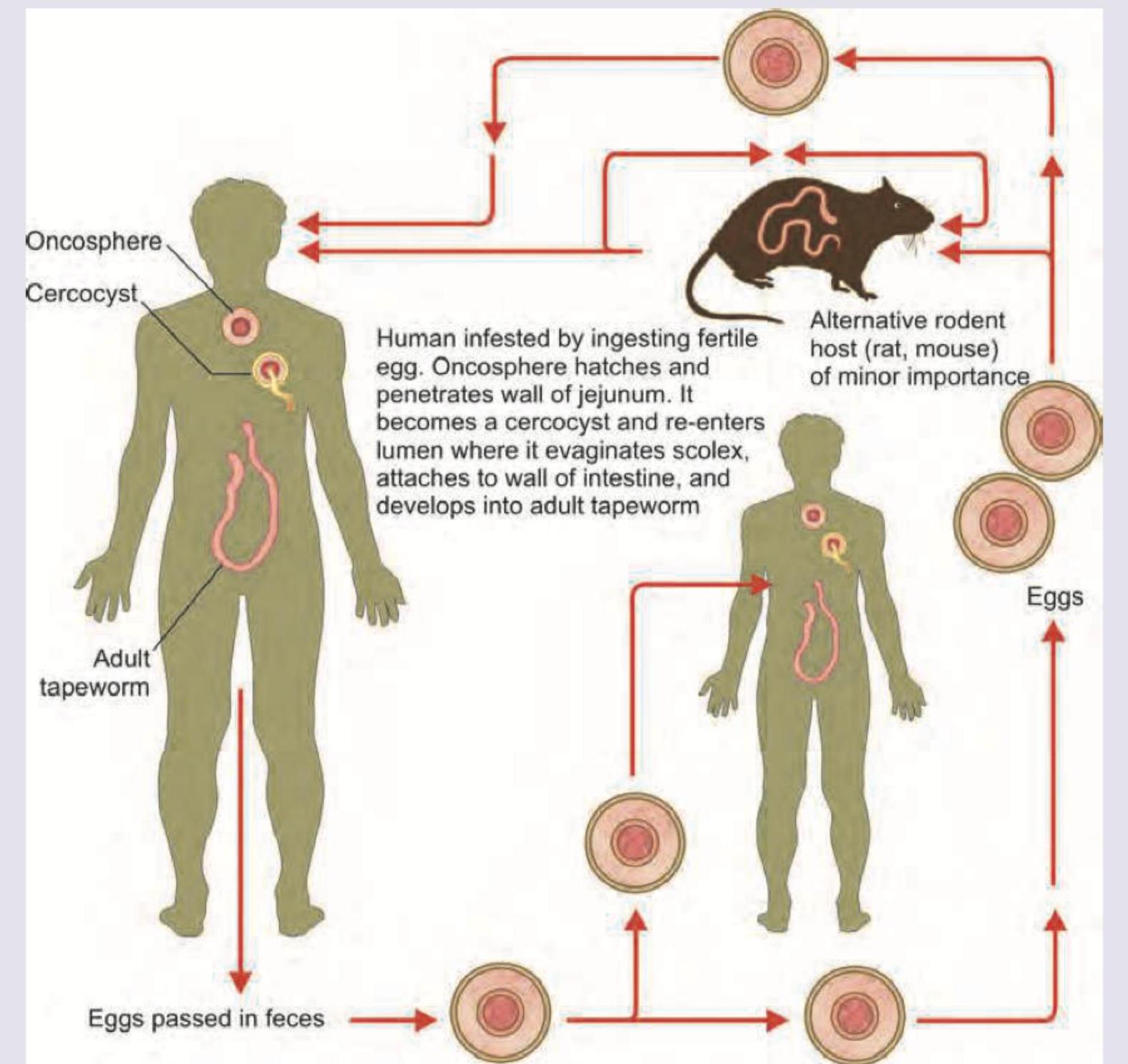
Which of the following fits into the life cycle of the picture given below? (AIIMS May 2017)
Which of the following parasite's life cycle is shown below?

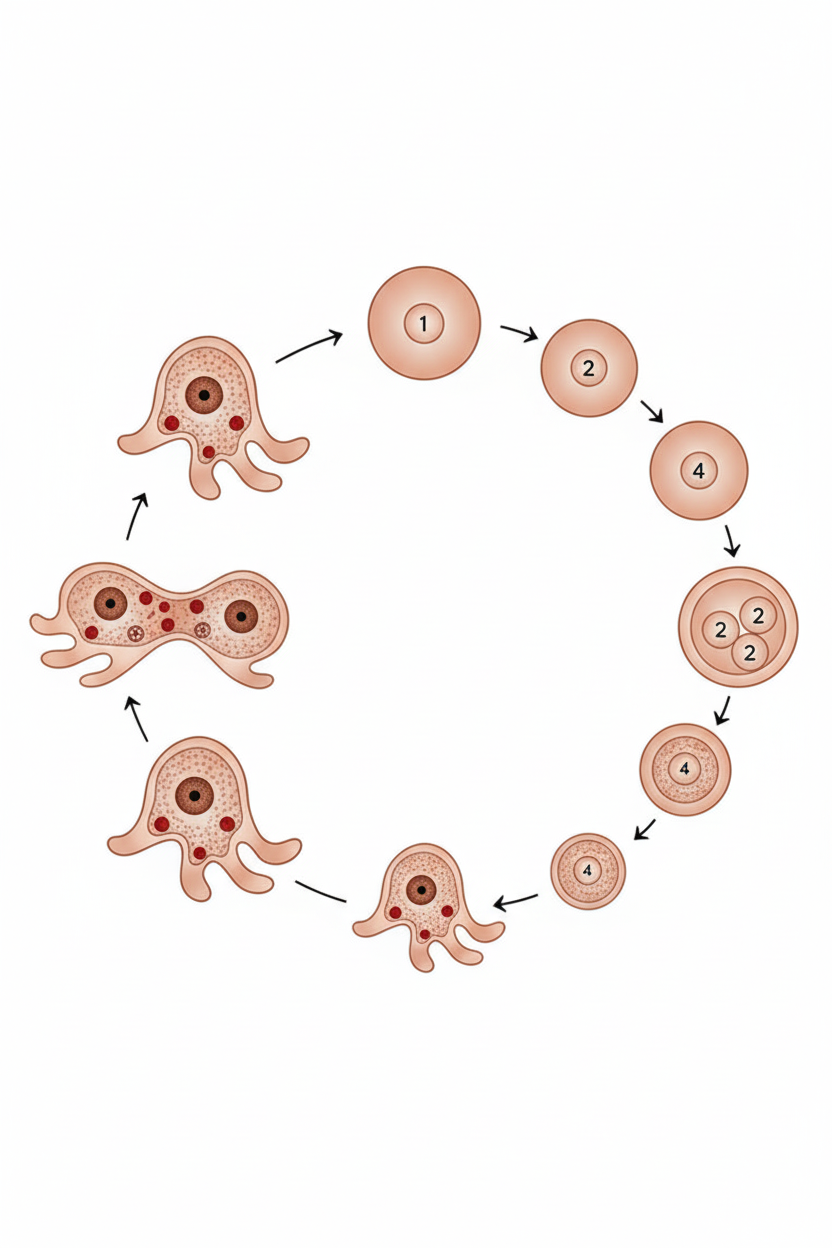
A 25-year-old man undergoes routine stool examination as part of a pre-employment health check. He is asymptomatic with no history of diarrhea or abdominal pain. Microscopy of the wet mount preparation (saline) shows the cyst form depicted in the image. Antigen detection testing is negative for Entamoeba histolytica-specific antigen. Identify the most likely organism.

Which of the following Schistosoma egg is shown below?

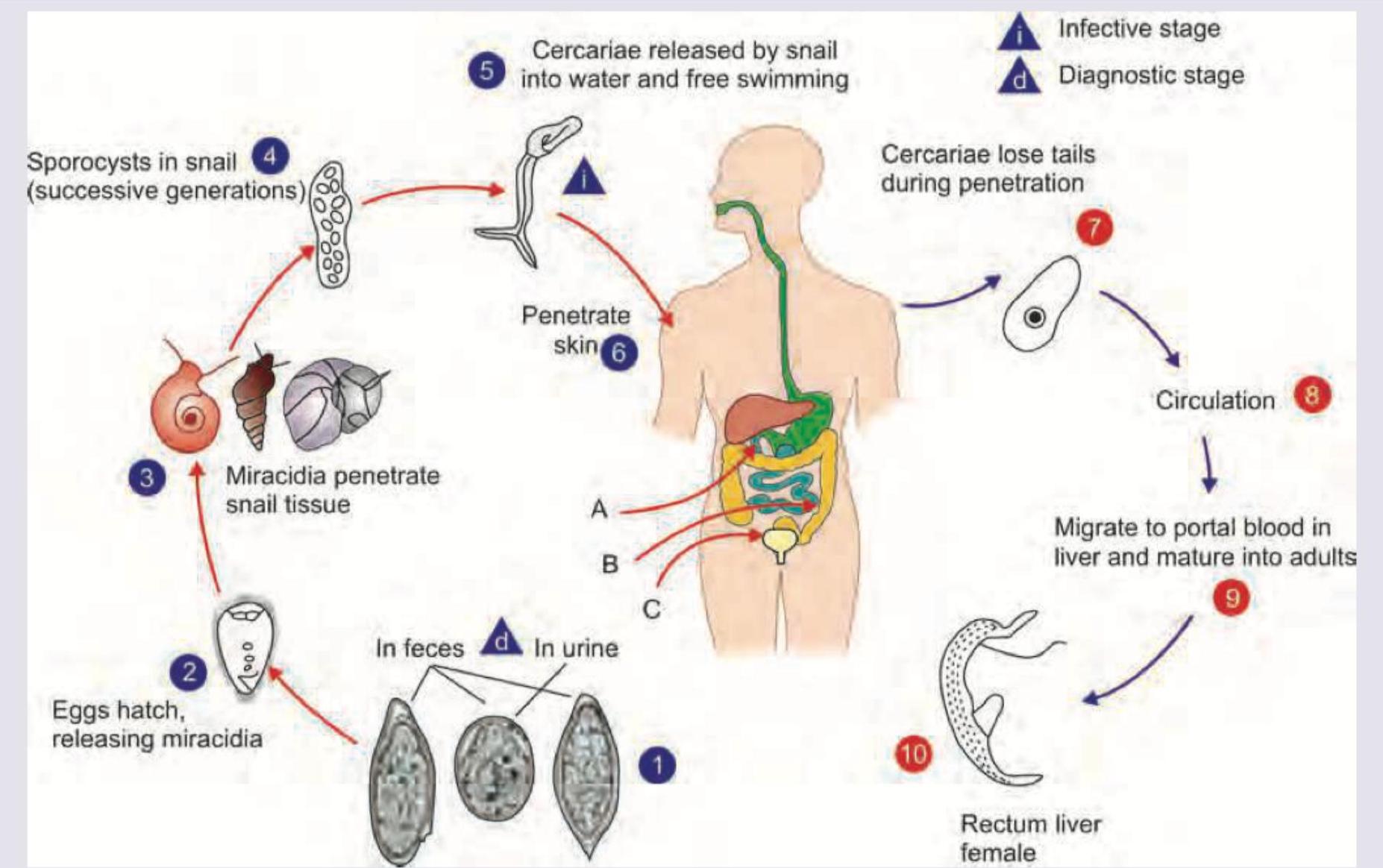
The life cycle shown in the image below is characteristic of which organism?
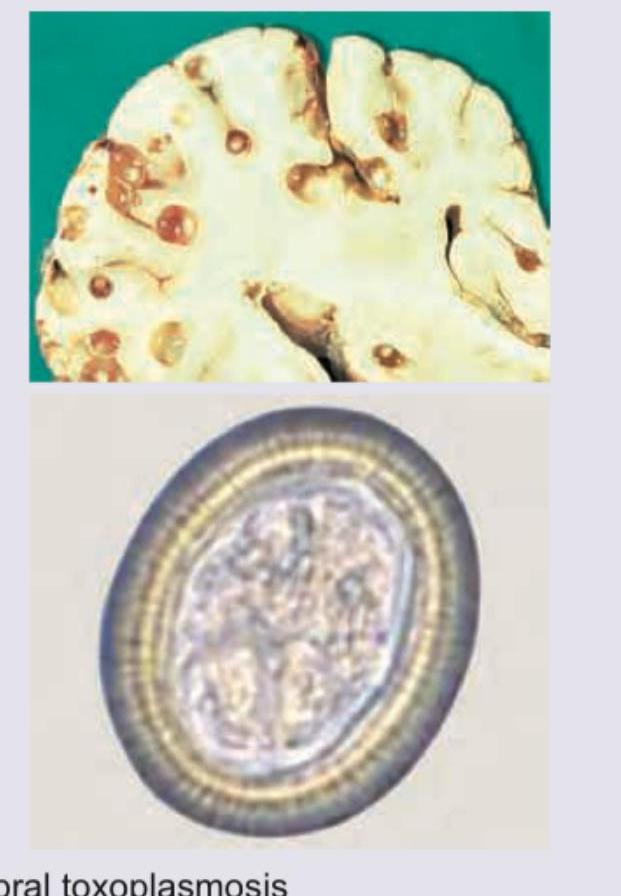
Which of the following CNS lesions is shown below?
Which of the following life cycles is shown below?
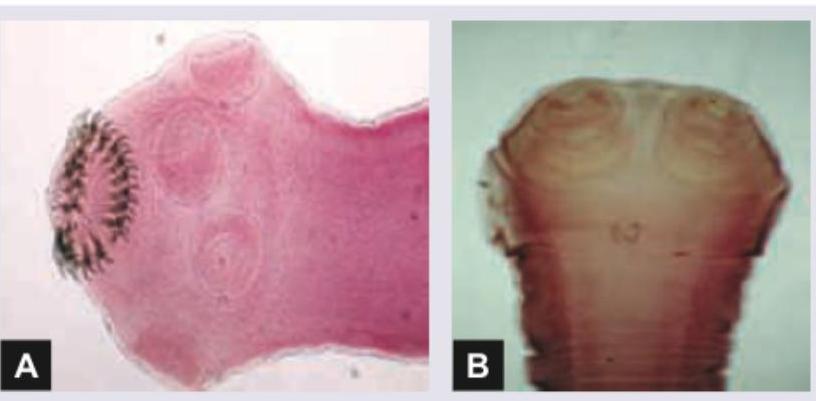
Which is correct of the parasite shown below?
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app