
Parasitology — MCQs

On this page
A 5-year-old child presents with nocturnal perianal itching. The image below shows the organism identified on an adhesive tape test. What is the most likely causative agent?
A diplomat from Peru was posted to India last week. Today he has brought his 10-year-old daughter to your clinic since the child has developed this swelling in the eye and feels feverish. Comment on the clinical sign and the insect bite responsible for the same:

Which of the following is correct about the image shown?

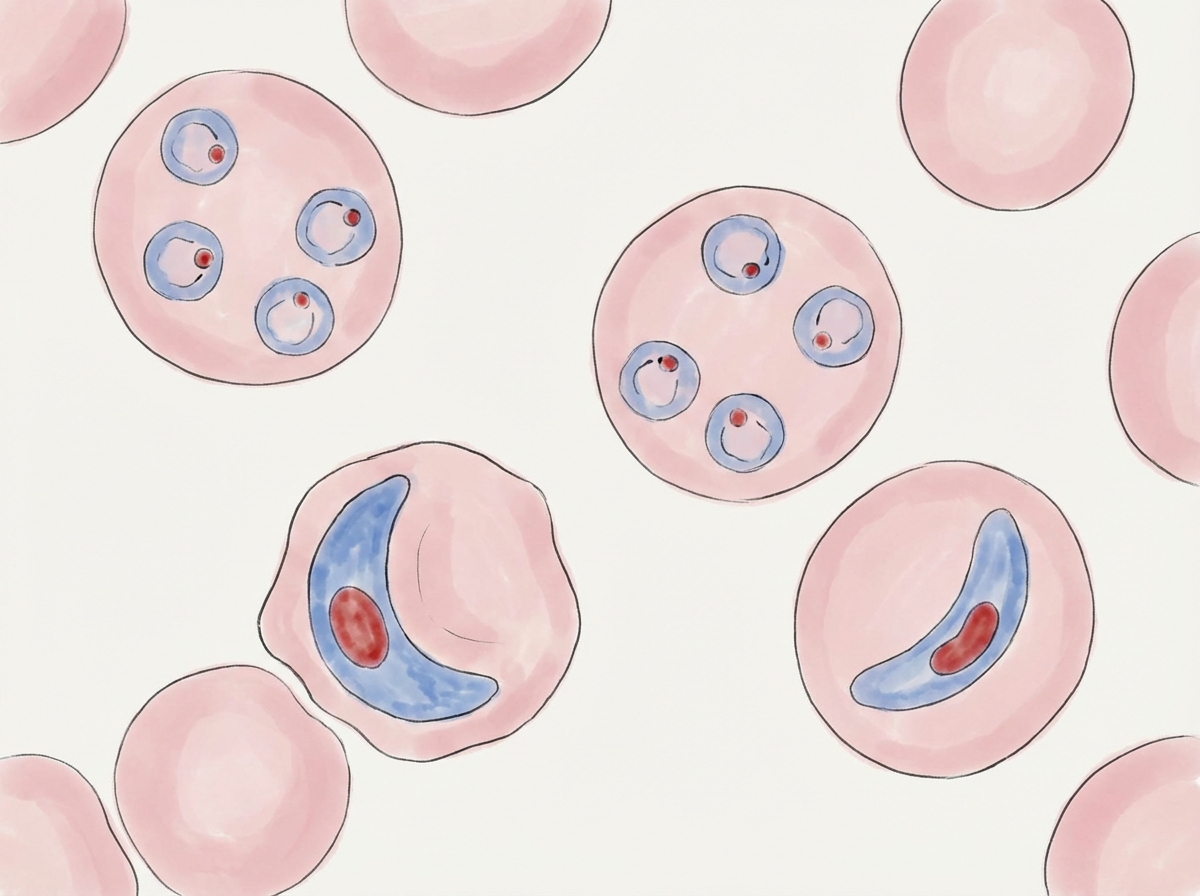
The following diagram depicts blood smear of which species?
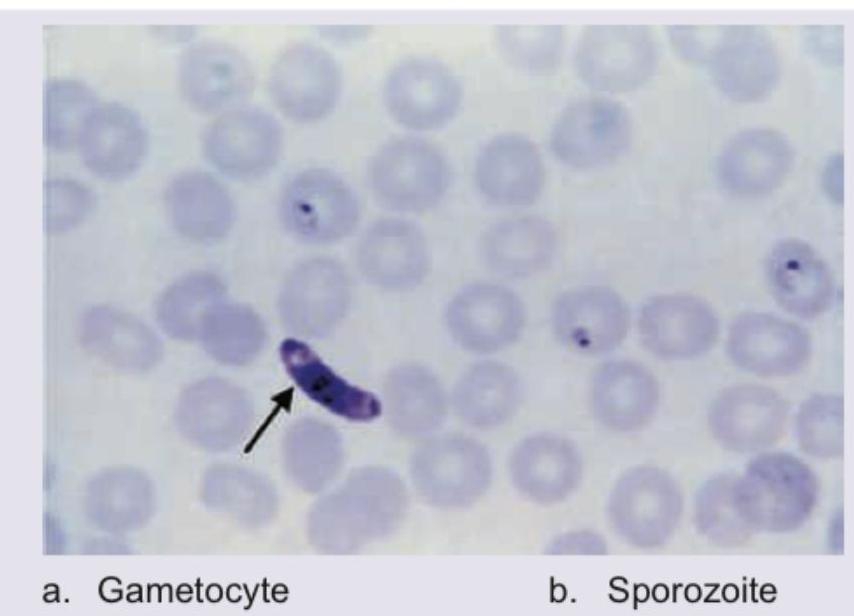
A 20-year-old lady presents with high grade fever and incoherent talking for 1 day. The following peripheral smear shows presence of:
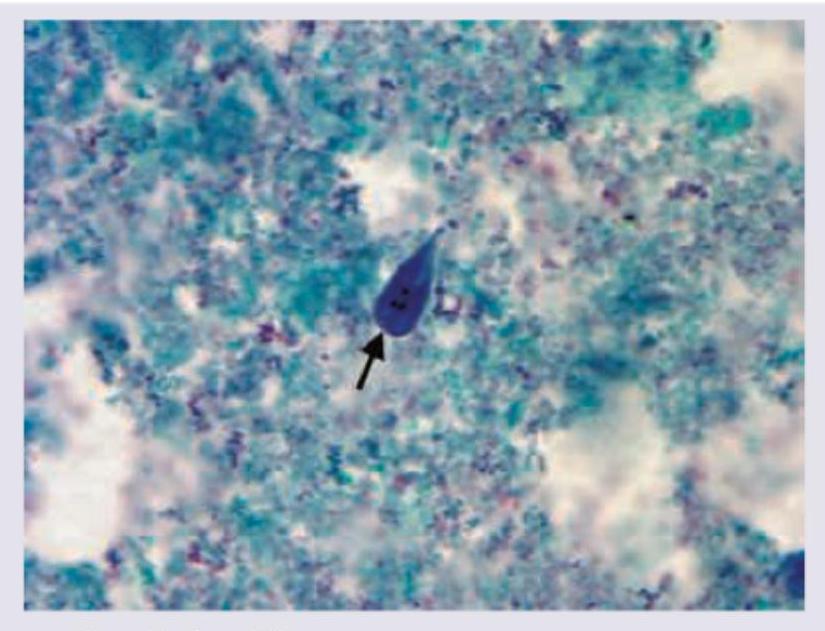
The image shows presence of:
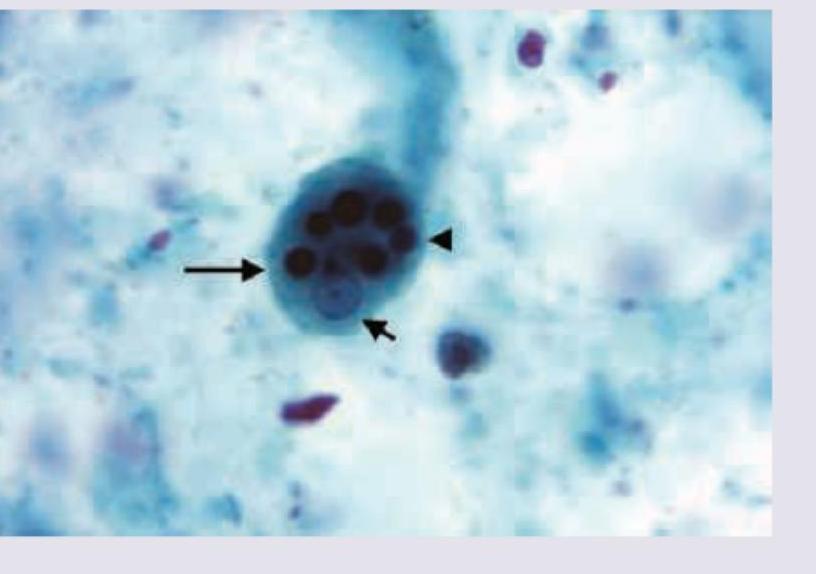
The following image shows presence of:
The following image shows presence of:

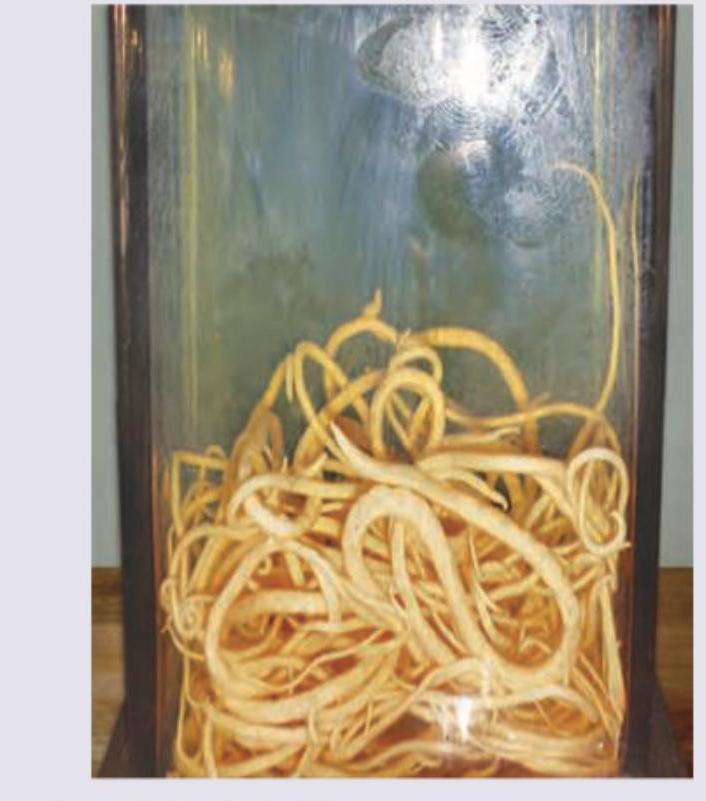
Which of the following worms is shown in the specimen?
Which of the following eggs is seen in stool microscope examination?

Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app