
Parasitology — MCQs

On this page
Which parasite commonly causes lung infestation?
Which of the following parasites can be found in ocular muscles?
Which disease is transmitted by sandflies?
Which parasite is associated with Charcot-Layden crystals but lacks pus cells in its stain?
A child presents with nocturnal perianal pruritus and adult worms in the stool. What is the most common intestinal infection in school-age children globally?
In which host is the adult worm of Echinococcus typically found?
Cysticercosis cellulosae causes infection with which of the following?
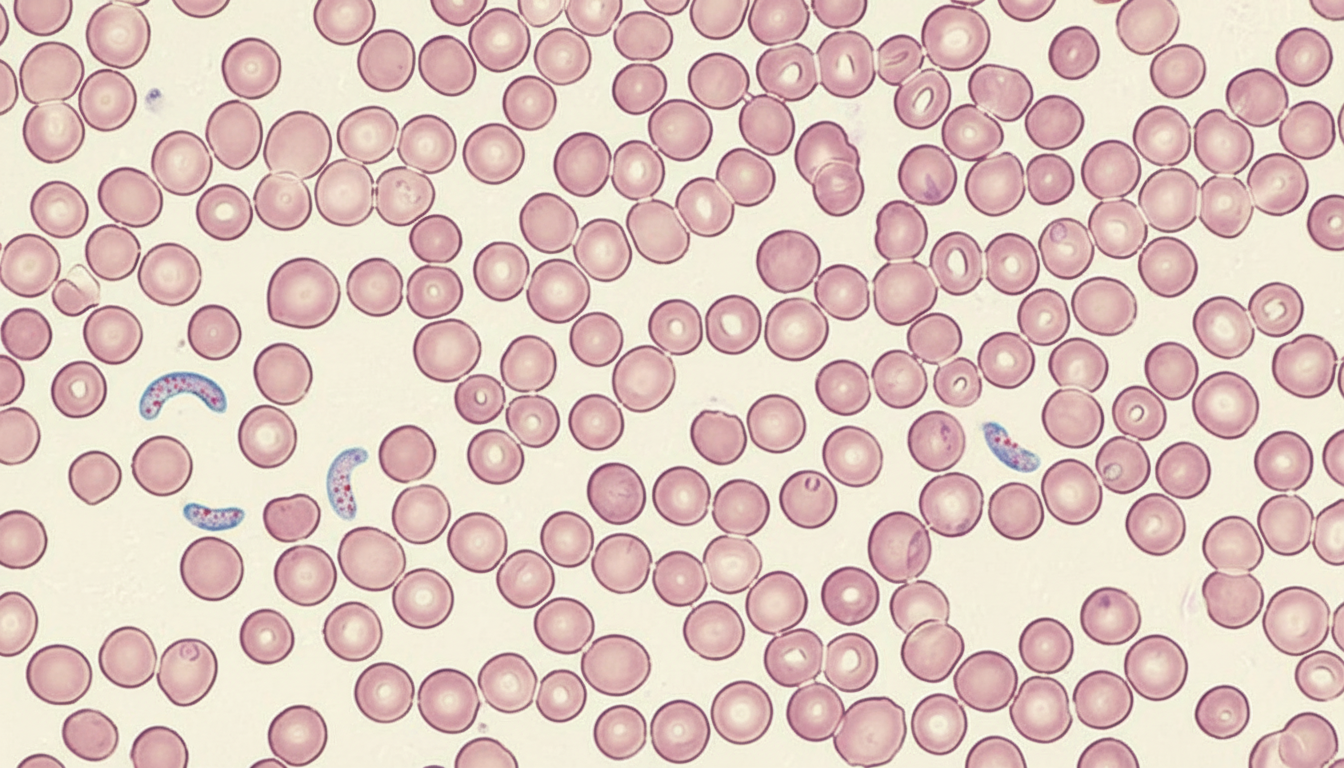
A 15-year-old boy presented with fever and chills for the last 3 days. A peripheral blood smear revealed the following. Which of the following is the most probable causative agent?
A 3-year-old child presents with weakness and a hemoglobin level of <5 gm/100 ml. There is a history of joint swelling and bleeding spots. What is the most likely causative organism?
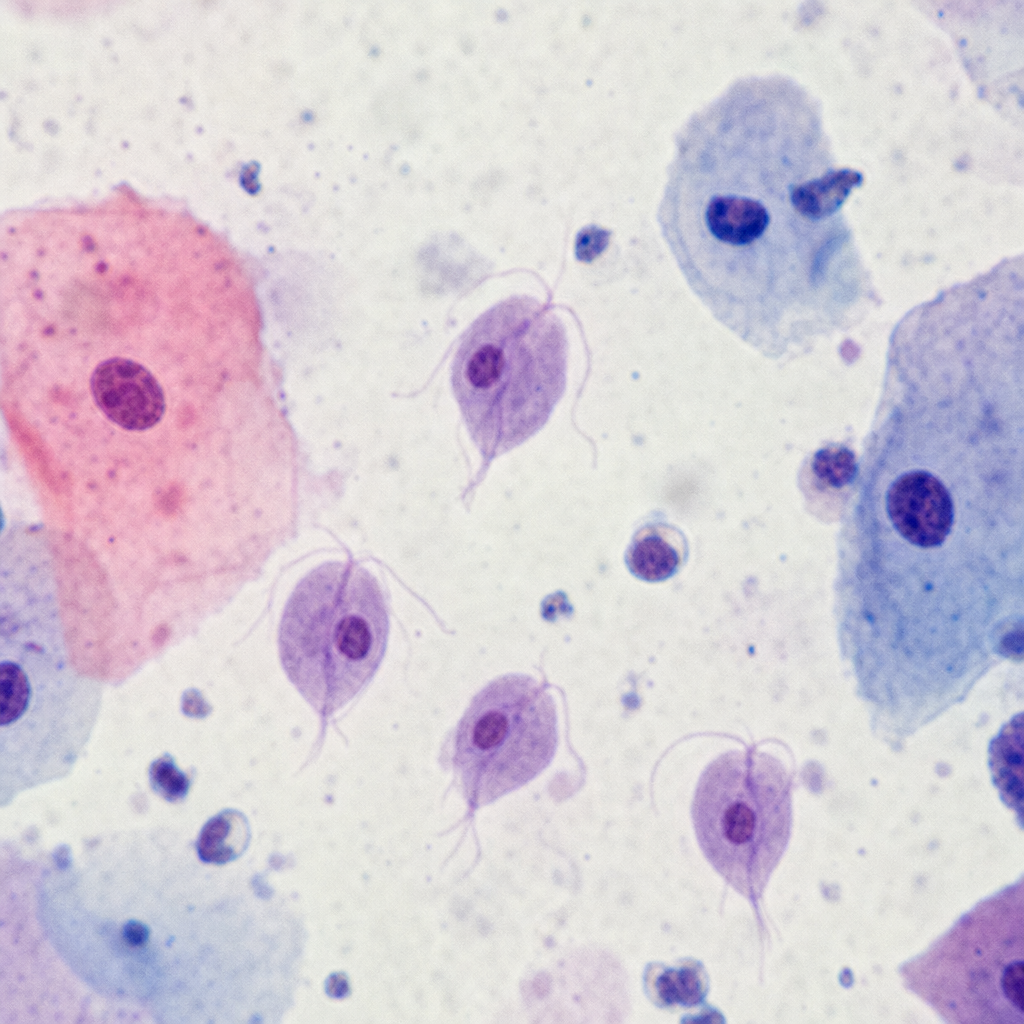
A 35-year-old lady presents with vaginal discharge. What is the likely causative organism seen on vaginal smears?
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app