
Parasitology — MCQs

On this page
Apart from Plasmodium, which of the following can infect red blood cells in ring forms?
Night blood survey is done in which of the following conditions?
Which of the following infections resembles malignancy?
Which of the following helminths primarily produces gastrointestinal symptoms, without lung involvement, during the course of its infection?
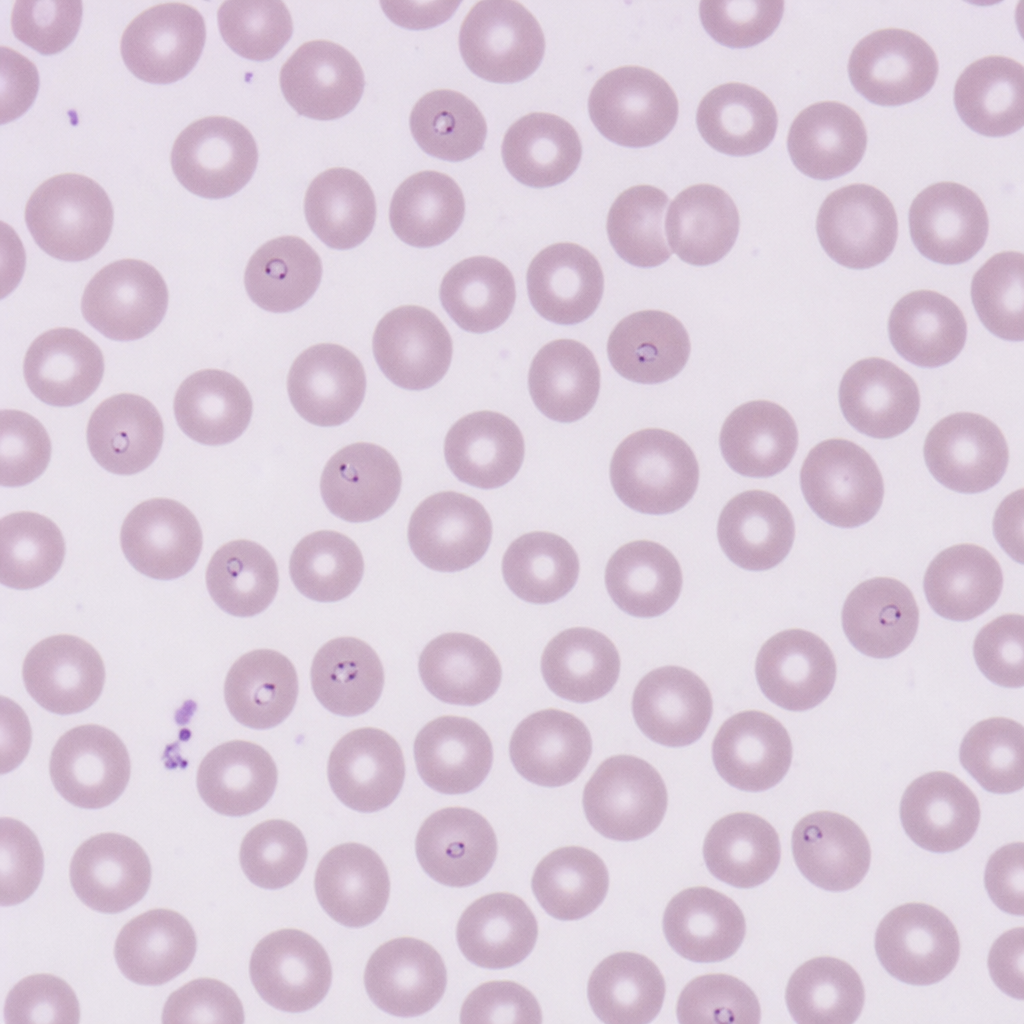
The provided diagram shows a blood smear. Which species of Plasmodium is depicted?
Which of the following acts as a reservoir for Toxoplasma gondii?
A 35-year-old man who recently traveled to a tropical country develops chronic, severe dysentery. Colonoscopy demonstrates ulceration of the cecum, and a cecal biopsy reveals 15-to-40 micron amoebae with ingested erythrocytes and small nuclei with distinctive tiny central karyosomes. Which of the following organisms is the most likely culprit?
What is the shortest incubation period in malaria?
A 26-year-old lady complains of discomfort during intercourse. Pelvic examination demonstrates a frothy, yellow-green vaginal discharge with a strong odour and small, red, ulcerations of the vaginal wall. A wet mount preparation demonstrates motile, flagellated protozoa. Which of the following is the most likely causative organism?
Which parasite commonly causes lung infestation?
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app