
Parasitology — MCQs

On this page
Where does Schistosoma Japonicum reside?
Splenic rupture is most commonly associated with infection by which of the following Plasmodium species?
'rK 39 antigen' is useful for the diagnosis of which condition?
The most sensitive among the following tests for the diagnosis of malaria is?
How is primary amoebic meningoencephalitis most likely acquired?
Which nematode resides in the caecum and appendix?
A man working in a construction company presented with watery, foul-smelling diarrhea since 3 weeks. There is no blood in the stools. If giardiasis is suspected, what is the best diagnostic method?
Which parasite commonly causes pulmonary eosinophilia syndrome?
What is the natural habitat of Schistosoma (blood flukes)?
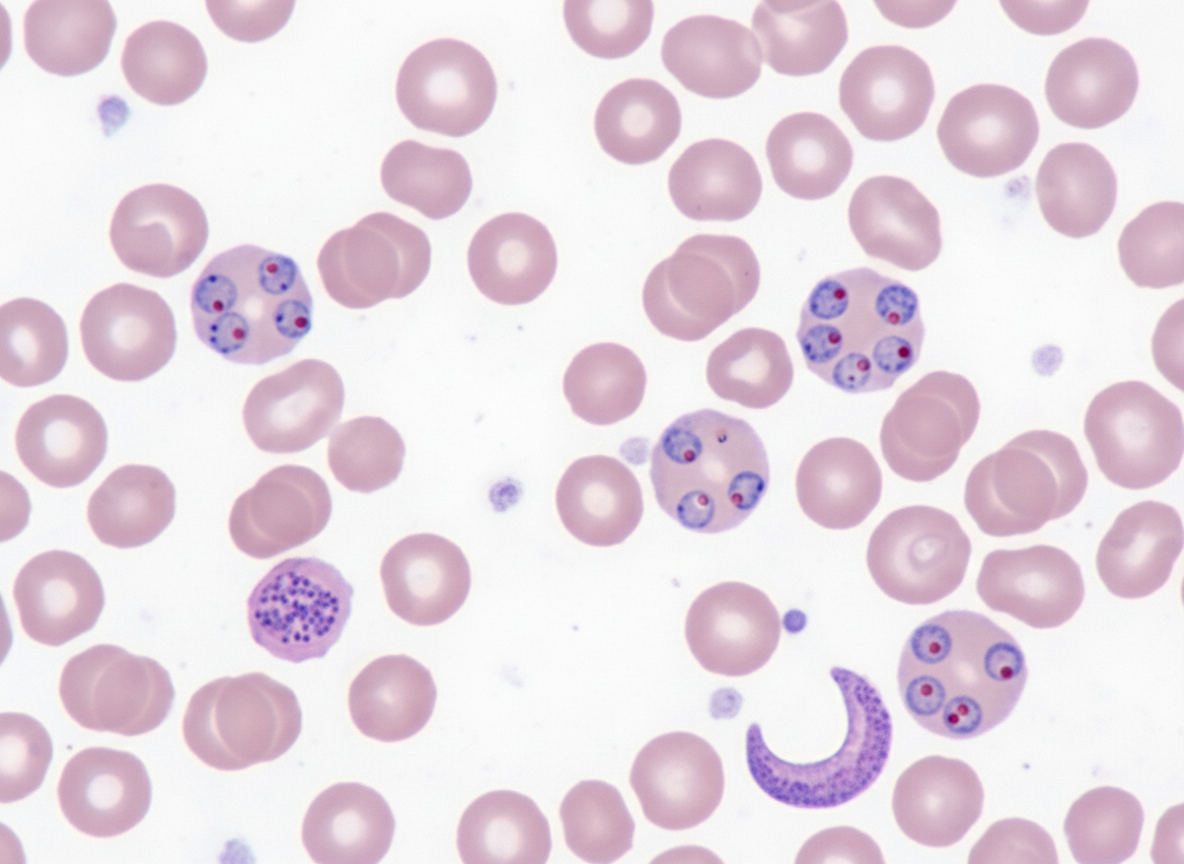
A patient from a tribal area of Jharkhand presents with fever for the last 3 days. Peripheral blood is collected and stained with Giemsa. A diagnosis of malaria is made. The smear is shown in the figure. What is the likely causative species?
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app