
Parasitology — MCQs

On this page
Lymphatic obstruction occurs with which of the following parasites?
Cutaneous larva currens is a feature of which of the following?
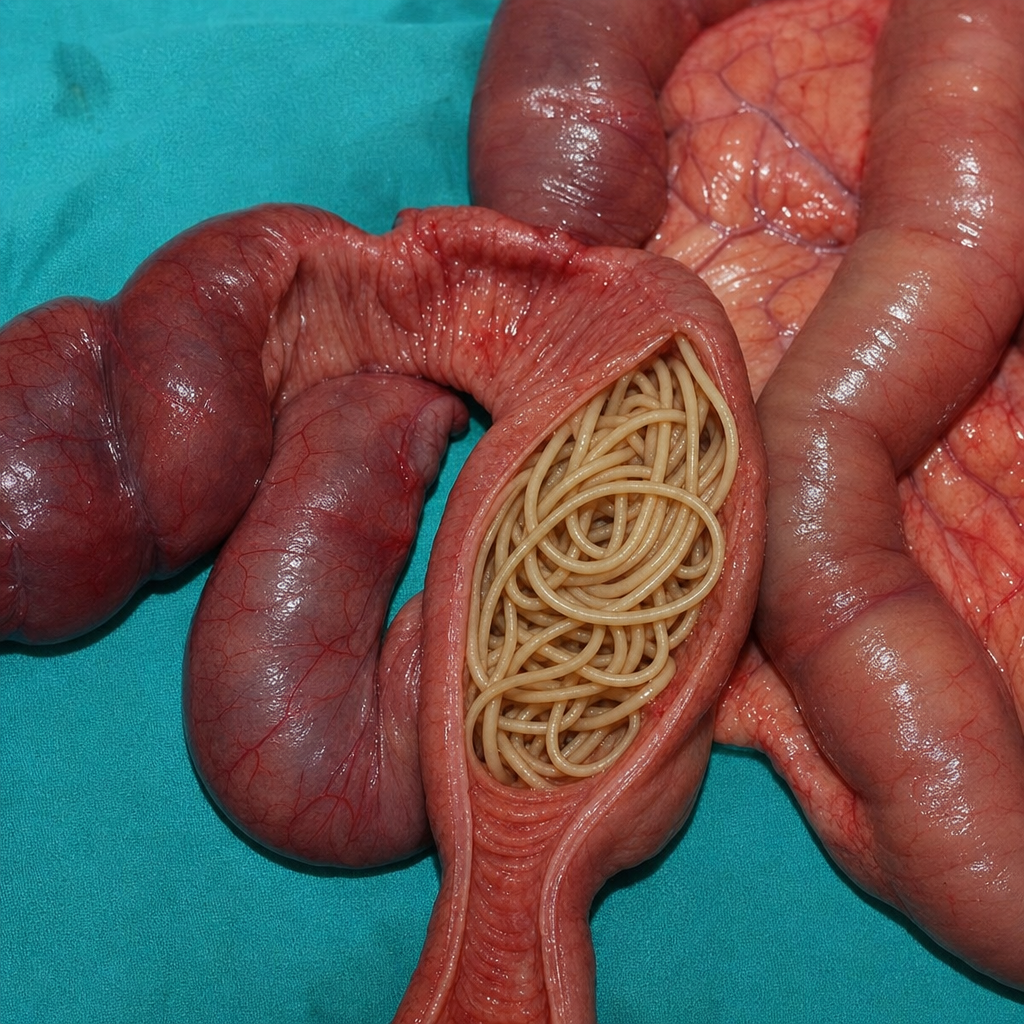
A specimen resected from a child with intestinal obstruction is shown. What is the most likely diagnosis?
In which host does the flagellar stage of the Leishmania parasite occur?
Which parasite causes biliary tract obstruction?
Which of the following statements regarding Malaria parasites is correct?
An AIDS patient presents with headaches and disorientation. A clinical diagnosis of Toxoplasma encephalitis is made, and Toxoplasma cysts are observed in a brain section. Which one of the following antibody results would be most likely in this patient?
Which of the following is NOT a recognized infectious cause of eosinophilia?
Which of the following statements about Giardiasis is FALSE?
In Plasmodium falciparum, how many cycles does the parasite undergo in the liver?
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app