
Parasitology — MCQs

On this page
What is typically true in large tapeworm infestations?
Ingested RBCs (erythrophagy) are seen in which of the following parasitic infections?
Which of the following statements about amoebiasis is NOT true?
Coconut cake appearance of the rectum is seen in which parasitic infection?
Calabar swellings are characteristic of infection with which parasite?
Cholangiocarcinoma has been associated with infection by which of the following organisms?
Which of the following is FALSE regarding Giardia lamblia?
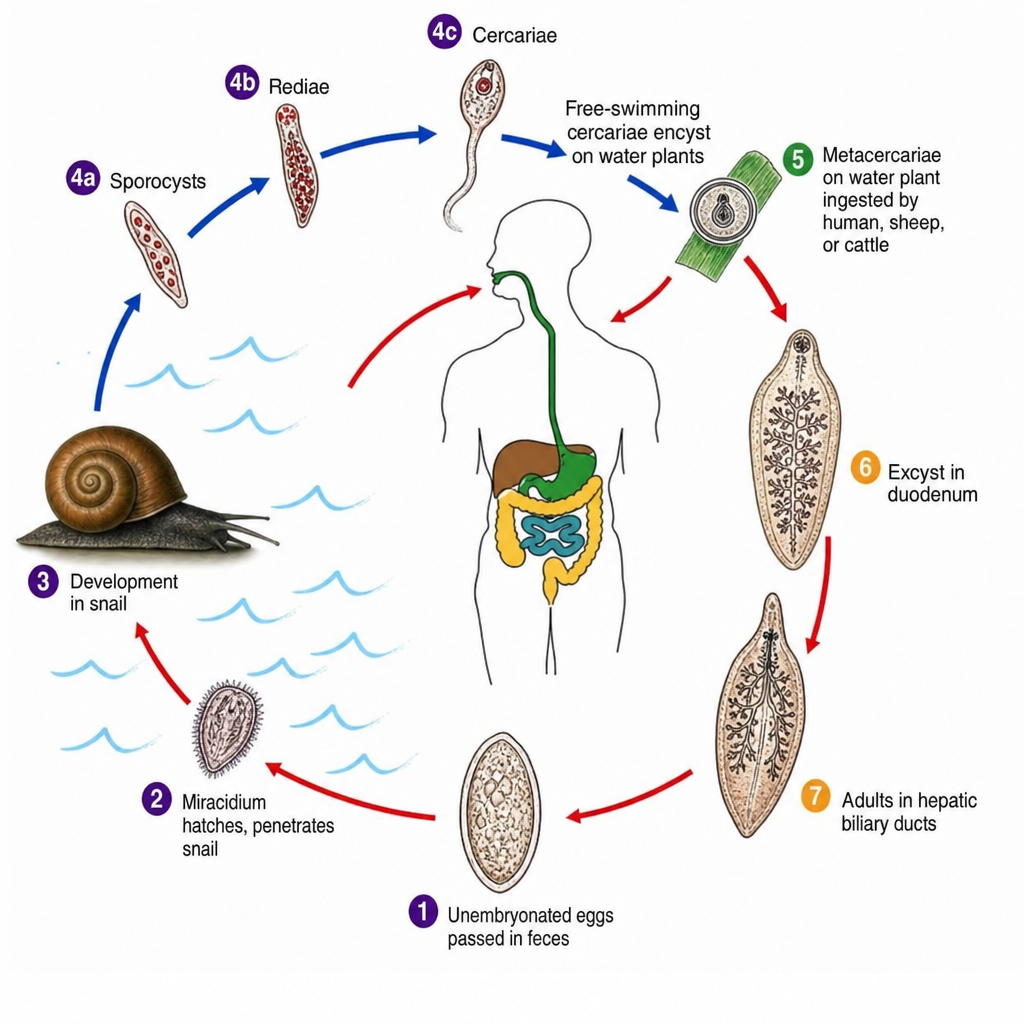
Which of the following parasite's life cycle is shown below?
Malaria recrudescence is defined as:
Which of the following is a true mode of transmission of Toxoplasma?
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app