
Parasitology — MCQs

On this page
Which of the following is NOT a true statement about filariasis?
An anxious mother brought her 4-year-old daughter to the pediatrician. The girl was passing loose stools for the past 20 days, often associated with abdominal pain. Stool examination showed the following organism:

Larvae of which of the following parasites reside in muscle tissue?
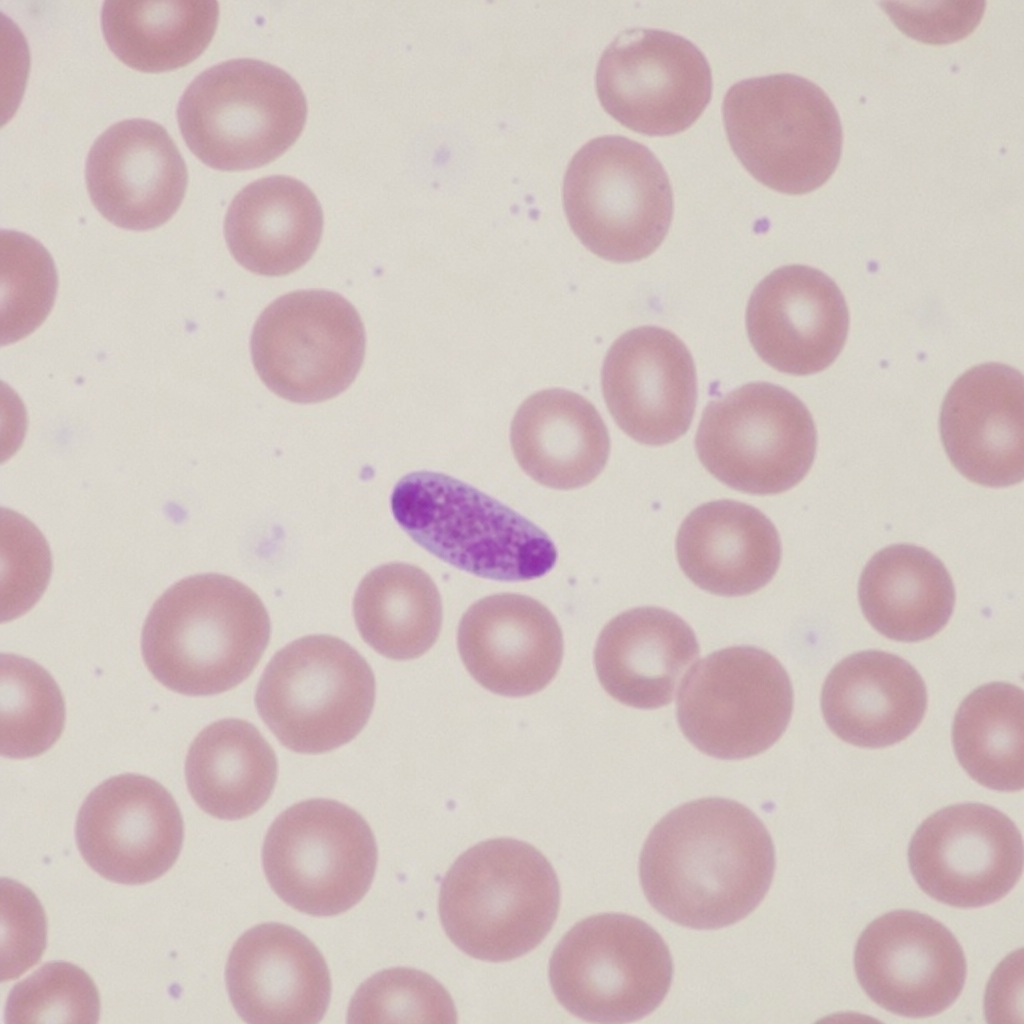
The following Peripheral Smear shows the presence of?
Profuse watery diarrhea in an immunocompromised child is due to which pathogen?
All of the following are true about amebic liver abscess except?
Which parasite causes lung cysts?
Transovarian transmission of infection occurs in which of the following vectors?
Which of the following is NOT associated with Loeffler's syndrome?
What is the causative agent of River blindness?
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app