
Parasitology — MCQs

On this page
An otherwise healthy person who wears contact lenses develops a small ulceration of the eye. What is the most likely cause?
Unsegmented eggs are seen in which of the following parasites?
A male patient presented with pain and discomfort in the upper abdominal region. His abdomen has enlarged, and he has experienced significant weight loss. The Casoni test is positive. What is the most likely diagnosis?
Napier's Aldehyde test is done for which of the following?
A 40-year-old male from Bihar complains of pain abdomen and has hepatosplenomegaly. A peripheral smear stain shows findings suggestive of which of the following parasitic infections?
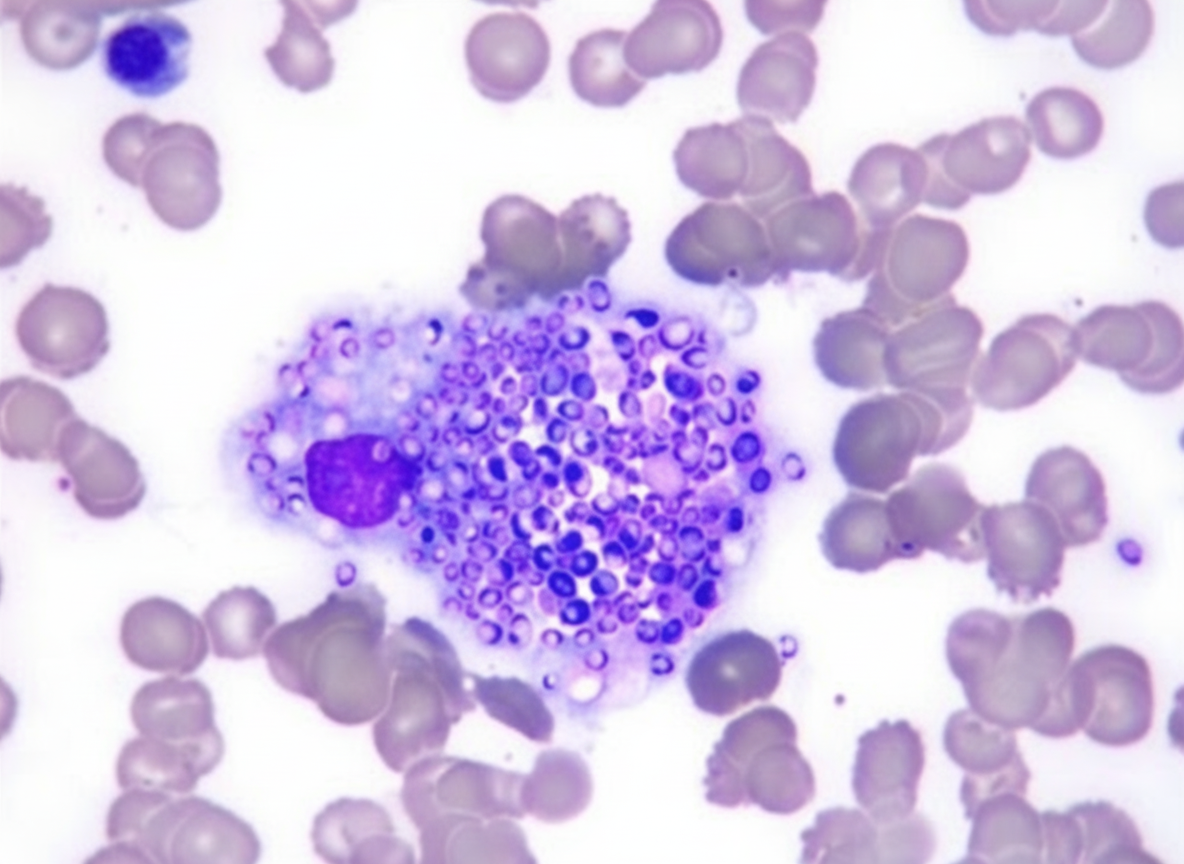
LD bodies are typically found in which stage of the Leishmania parasite lifecycle?
Which of the following helminth eggs are typically non-bile stained?
The image shows the ovum of a helminth. What is true about this helminth?

Which of the following parasites can be detected in a peripheral blood smear?
Which of the following methods is used to diagnose a corneal ulcer caused by Acanthamoeba?
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app