
Parasitology — MCQs

On this page
What is true about the peripheral blood smear of Plasmodium vivax?
Which of the following parasitic infections is associated with Salmonella?
A girl complained of abdominal pain with the passage of foul-smelling stool that does not wash away easily. There is a history of swimming in contaminated water. What is the likely causative organism?
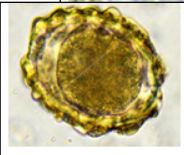
A stool sample from a patient shows ova. How do humans typically acquire this parasitic infection?
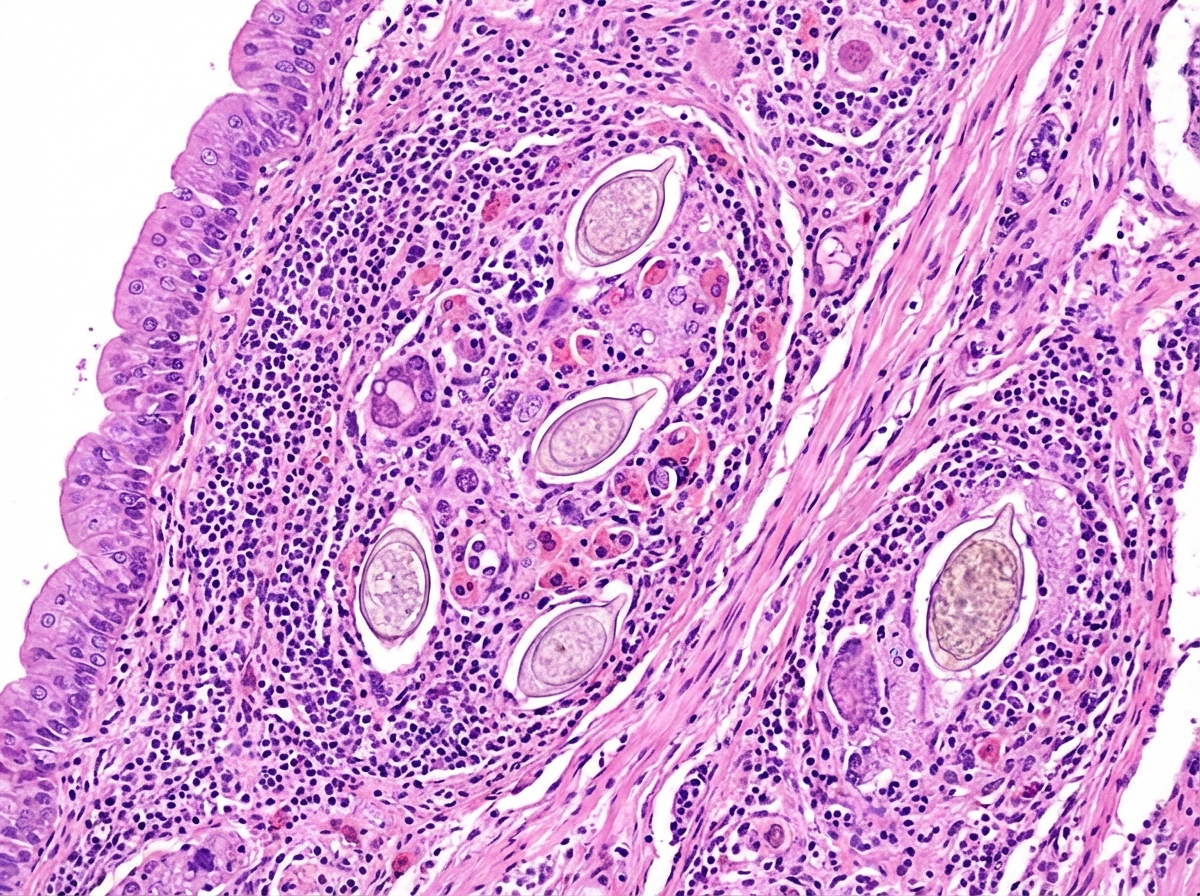
A 35-year-old male presented with gross hematuria, with similar episodes occurring in the past 6 months. There was no history of fever, pain, or burning on urination, weight loss, or increased sense of urgency to void. There was no history of exposure to toxins either at work or during recreational activities. He had a history of swimming in freshwater lakes in sub-Saharan Africa 2 years prior. The patient underwent fiberoptic cystoscopy, and a mass was noted in the fundus of the bladder. Biopsy of the mass is shown in the figure. What is the drug of choice for the likely cause?
The man-snail-crab life cycle is characteristic of which parasite?
Which of the following is NOT true about Plasmodium falciparum?
Babesiosis is transmitted by the bite of which arthropod?
Which of the following inhibits digestion in the intestinal mucosa?
Which of the following is NOT a cause of malabsorption?
Practice by Chapter
Classification of Parasites
Practice Questions
Intestinal Protozoa
Practice Questions
Blood and Tissue Protozoa
Practice Questions
Malaria Parasites
Practice Questions
Leishmaniasis
Practice Questions
Intestinal Helminths: Nematodes
Practice Questions
Tissue Nematodes
Practice Questions
Trematodes
Practice Questions
Cestodes
Practice Questions
Ectoparasites
Practice Questions
Antiparasitic Drugs
Practice Questions
Laboratory Diagnosis of Parasitic Infections
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app