
Venerology — MCQs

On this page
A 40-year-old man presents with a 2-week history of a non-tender penile ulcer. Dark field microscopy is negative, and initial VDRL is non-reactive. What is the most appropriate next step?
Which of the following is a defining characteristic of Lymphogranuloma venereum (LGV)?
A 23-year-old woman presents with recurrent genital herpes despite continuous suppressive therapy with valacyclovir 1g daily for 6 months. She reports adherence to medication. HIV test is negative. What is the most appropriate next step in management?
A 35-year-old HIV-positive woman (CD4 count 320/μL) presents with extensive genital warts not responding to conventional treatments. Which of the following is the most appropriate management?
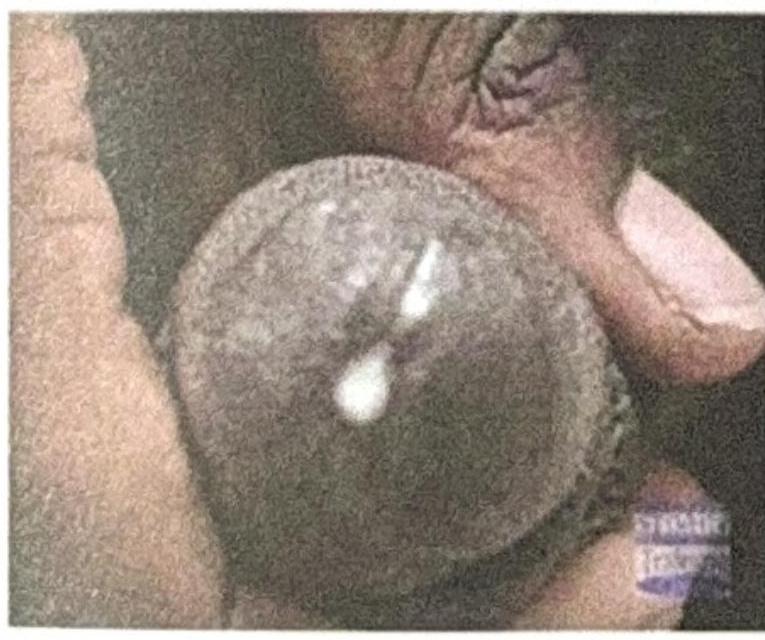
A male presents with urethral discharge as shown in the figure. What is the most likely cause?
A 28-year-old man presents with painless anal ulcer. Dark-field microscopy shows spirochetes. He is allergic to penicillin with history of anaphylaxis. Which of the following is the most appropriate treatment?
A 42-year-old man presents with painless penile ulcer and rash on palms and soles. VDRL is positive at 1:64. CSF examination shows: WBC 35/μL (lymphocytes), protein 65 mg/dL, VDRL positive. Which of the following is the most appropriate treatment?
Which diagnostic test is most appropriate for detecting early congenital syphilis?
What is the most common cause of genital ulcers globally?
A 40-year-old female with multiple sexual partners presented with fever, rash, and articular symptoms. Migratory arthritis and tenosynovitis of knees, hands, wrists, feet, and ankles were noticed during clinical examination. Synovial fluid leukocyte count was 12,000/ml and culture was sterile. The patient has been successfully treated with injection ceftriaxone 1 g Q24 hours for 7 days. What was the diagnosis in this setting?
Practice by Chapter
Syphilis
Practice Questions
Gonorrhea
Practice Questions
Chlamydial Infections
Practice Questions
Chancroid and Other Genital Ulcers
Practice Questions
Genital Herpes
Practice Questions
Human Papillomavirus Infections
Practice Questions
HIV and STIs
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
STI Screening and Prevention
Practice Questions
Partner Notification and Treatment
Practice Questions
Sexually Transmitted Enteric Infections
Practice Questions
Special Populations Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app