
Venerology — MCQs

On this page
A 25-year-old male presents with a burning sensation during urination and purulent discharge from the penis, which started 5 days ago. He reports unprotected sexual intercourse with a new partner two weeks ago. Examination reveals an erythematous urethral meatus with noticeable purulent discharge. A Gram stain of the discharge reveals intracellular gramnegative diplococci. The patient is otherwise healthy with no known drug allergies. What is the most appropriate treatment for this patient?
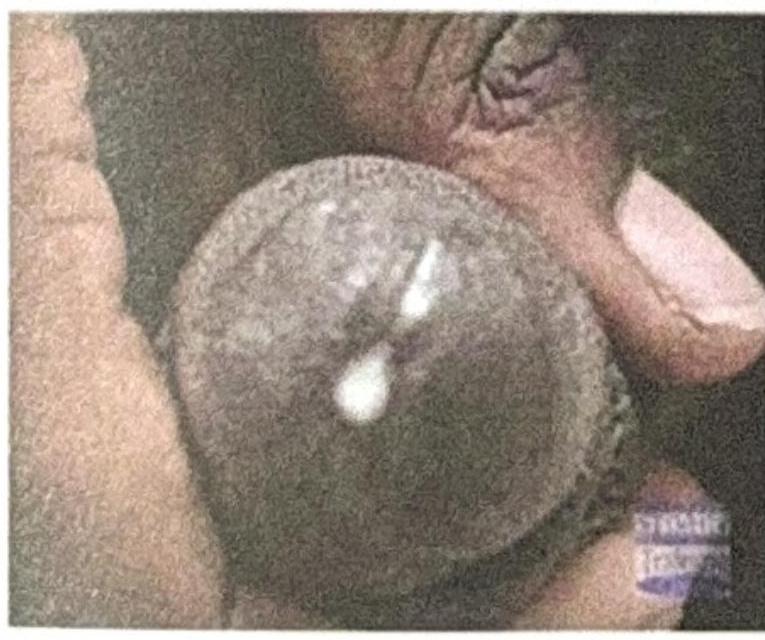
A male presents with urethral discharge as shown in the figure. What is the most likely cause?
A 28-year-old man presents with painless anal ulcer. Dark-field microscopy shows spirochetes. He is allergic to penicillin with history of anaphylaxis. Which of the following is the most appropriate treatment?
A 25-year-old woman presents for STI screening. She reports consistent condom use with her partner. Which of the following STIs is least effectively prevented by proper condom use?
A 42-year-old man presents with painless penile ulcer and rash on palms and soles. VDRL is positive at 1:64. CSF examination shows: WBC 35/μL (lymphocytes), protein 65 mg/dL, VDRL positive. Which of the following is the most appropriate treatment?
A 35-year-old man presents with burning penile lesions 3 days after unprotected intercourse. He has no prior history of similar lesions. Which of the following best differentiates primary from recurrent HSV infection?
A 45-year-old man presents with a 2-month history of painless testicular swelling. He reports being treated for syphilis 20 years ago. Examination reveals bilateral, non-tender testicular enlargement. Which of the following is the most likely diagnosis?
A 30-year-old man presents with generalized lymphadenopathy, palmar rash, and condylomata lata 2 months after being treated for primary syphilis. VDRL is positive at 1:128. Which of the following best explains the pathogenesis of these manifestations?
A 19-year-old woman presents for STI screening. She is asymptomatic but reports multiple sexual partners. Which of the following screening tests should be performed according to current guidelines?
A 24-year-old man presents with dysuria and urethral discharge 5 days after unprotected sexual intercourse. Gram stain of the discharge shows intracellular gram-negative diplococci. The patient reports penicillin allergy. Which of the following is the most appropriate empiric treatment?
Practice by Chapter
Syphilis
Practice Questions
Gonorrhea
Practice Questions
Chlamydial Infections
Practice Questions
Chancroid and Other Genital Ulcers
Practice Questions
Genital Herpes
Practice Questions
Human Papillomavirus Infections
Practice Questions
HIV and STIs
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
STI Screening and Prevention
Practice Questions
Partner Notification and Treatment
Practice Questions
Sexually Transmitted Enteric Infections
Practice Questions
Special Populations Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app