
Pulmonology — MCQs

On this page
A patient with limited systemic sclerosis for the past 10 years complains of shortness of breath for the past one year. His pulmonary function tests are as follows: FVC 2.63 (predicted 2.82), FEV1 88% of predicted, and DLCO 5.2 (predicted 16.3). Which among the following is the probable diagnosis?
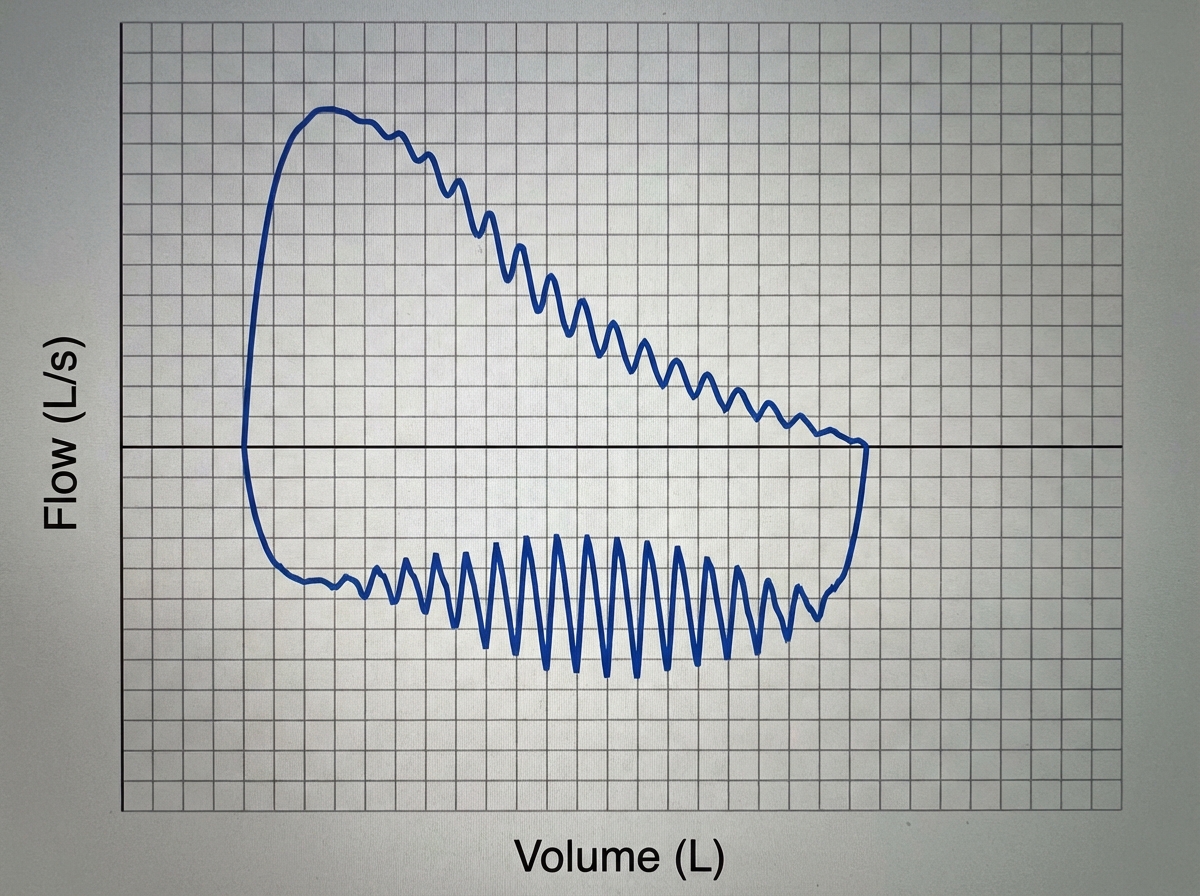
What is the probable diagnosis in a patient with ptosis, fatigable bulbar weakness, and the following flow-volume loop after spirometry?
A 29-year-old unmarried female presents with dyspnea. Her chest X-ray is normal, FVC is 92%, FEV1/FVC is 89%, and DLCO is 59% of normal. On exercise, her oxygen saturation drops from 92% to 86%. What is the likely diagnosis?
Which of the following conditions are associated with transudative pleural effusion?
Pleural fluid with low glucose is seen in all of the following conditions EXCEPT?
A 45-year-old female presents with hemoptysis and cough. The hemoptysis started 2 weeks ago, followed by fever and cough. X-rays showed left upper lobe consolidation. Antibiotics were administered. The fever improved, but the cough and hemoptysis persisted. BP 110/72 mmHg, Pulse 70/min. Bronchoscopy shows a mass filling the left bronchus. What is the likely diagnosis?
Which of the following statements is FALSE regarding Idiopathic Pulmonary Fibrosis?
Recognized features of asbestosis do not include which of the following?
Pneumatoceles are seen in which of the following conditions?
Bronchiectasis with predominantly upper lobe involvement is characteristic of which condition?
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app