
Neurology — MCQs

On this page
A 58-year-old woman with a history of alcohol abuse, coronary artery disease, and atrial fibrillation is on metoprolol, lisinopril, simvastatin, and warfarin. She develops urinary urgency and frequency and is treated with oxycodone and ciprofloxacin. Three days later, she develops a headache, dizziness, vomiting, and difficulty walking. Neurological examination reveals normal strength, sensation (including vibratory sensation), and reflexes. She has an uncoordinated, unsteady gait. Testing of coordination in the upper extremities shows past pointing and poor rapid alternating movements with her right upper extremity. In the lower extremities, her heel-shin testing also reveals poor coordination on the right. Her INR is 6.5 (normal <1; therapeutic for warfarin is 2.0-3.0). What is the most likely cause of her neurologic findings?
Which of the following is used in the acute exacerbation of multiple sclerosis?
What is the most common cause of death in measles?
An 80-year-old chronic alcoholic was diagnosed with atrial fibrillation five years ago. His son describes a stepwise decline in his father's overall memory over these years. On examination, he is having pseudobulbar affect with brisk deep tendon reflexes in the left upper extremity and up-going plantars. What is the diagnosis?
Limbs elevated against gravity but not against resistance is which grade of muscle power?
What is the investigation of choice for the diagnosis of epilepsy?
Which condition shows characteristic EEG findings of 3 Hz generalized spike and wave discharges?
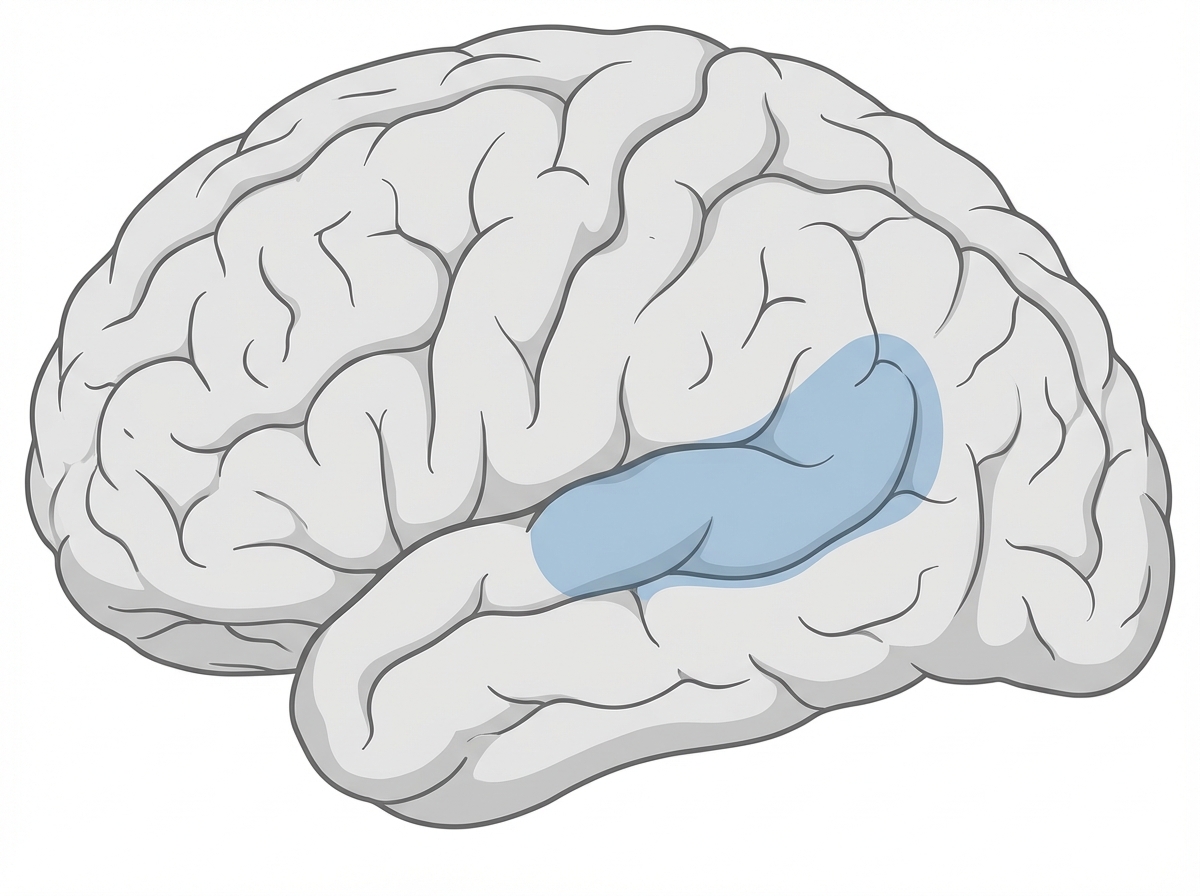
Which of the following is likely to be found in a patient with a lesion in the shaded area?
Anti-GD1 antibodies are seen in which variant of Guillain-Barré syndrome?
Which condition is associated with a characteristic EEG finding?
Practice by Chapter
Cerebrovascular Diseases
Practice Questions
Seizure Disorders and Epilepsy
Practice Questions
Headache Disorders
Practice Questions
Movement Disorders
Practice Questions
Demyelinating Diseases
Practice Questions
Neurodegenerative Disorders
Practice Questions
Neuromuscular Junction Disorders
Practice Questions
Peripheral Neuropathies
Practice Questions
CNS Infections
Practice Questions
Neuro-oncology
Practice Questions
Dementia and Cognitive Disorders
Practice Questions
Neurological Emergencies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app