
Neurology — MCQs

On this page
A female presented with a severe headache of sudden onset. On CT scan, a diagnosis of subarachnoid hemorrhage is made. What is the most common cause of subarachnoid hemorrhage?
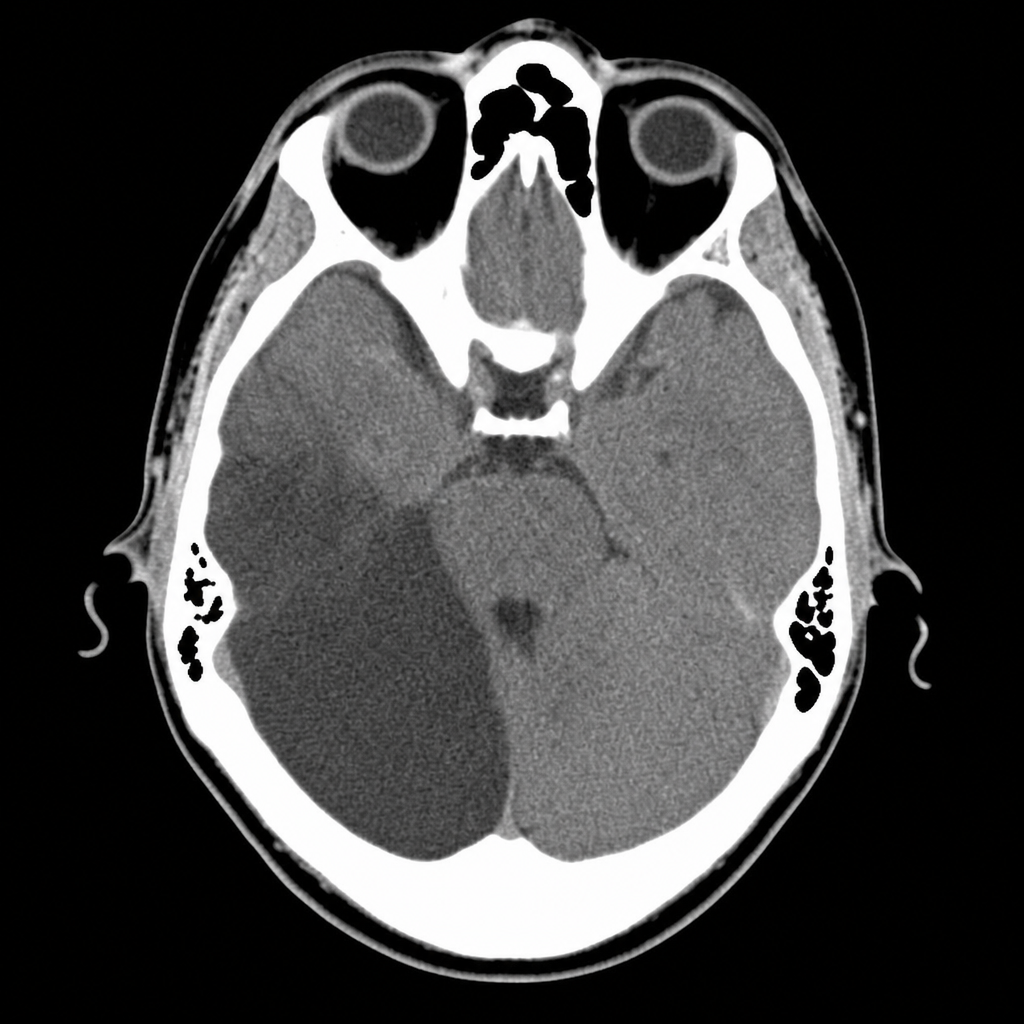
A 58-year-old male presents with a history of ipsilateral facial paralysis and contralateral hemiplegia. A plain CT scan of the head is provided. What is the most likely diagnosis?
Which type of headache typically affects young to middle-aged men, is unilateral, oculo-temporal, excruciating, and associated with lacrimation and rhinorrhoea?
Hemiplegia is commonly associated with infarction of the area of distribution of which artery?
Deep brain stimulation is used in the treatment of which of the following conditions?
A 25-year-old weightlifter experienced a severe headache during training. A CSF tap performed on the medical ward showed blood stains. What is the likely diagnosis?
Which reflex is being tested?

Raised intracranial pressure will cause which of the following?
A patient appears awake but is not talking and has no voluntary movements. The patient can signal with vertical eye movements. A CT scan shows infarction of the ventral pons. What is the most likely diagnosis?
The above marked structures are seen in a condition where the most common cause of death is?

Practice by Chapter
Cerebrovascular Diseases
Practice Questions
Seizure Disorders and Epilepsy
Practice Questions
Headache Disorders
Practice Questions
Movement Disorders
Practice Questions
Demyelinating Diseases
Practice Questions
Neurodegenerative Disorders
Practice Questions
Neuromuscular Junction Disorders
Practice Questions
Peripheral Neuropathies
Practice Questions
CNS Infections
Practice Questions
Neuro-oncology
Practice Questions
Dementia and Cognitive Disorders
Practice Questions
Neurological Emergencies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app