
Infectious Diseases — MCQs

On this page
Which of the following diseases is commonly referred to as 'breakbone fever'?
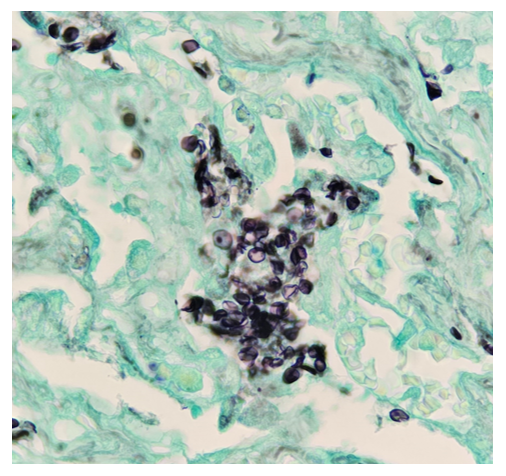
A 44-year-old female presented to OPD with complaints of pallor, fatigue, weakness, palpitations and dyspnea on exeion. Blood tests were conducted, which revealed, Anemia Thrombocytopenia Leukocytosis with neutropenia and increased blasts in the peripheral blood smear. Peripheral blood smear The patient was diagnosed with leukemia and she underwent allogenic stem cell transplantation for the same. After 24 days, she again presented with hypotension, tachycardia, and spO2 of 88% along with a new rash from which biopsy was taken and silver staining was done. Lab findings revealed severe Neutropenia. Which is the most likely organism causing the above skin condition: -
Which of the following is true of typhoid?
The spike of fever in malaria is at the time of release of ?
Major signs for AIDS case definition according to WHO is-
One of your staff nurses sustained a deep needle stick injury from a needle used to inject an HIV positive individual. What is the treatment regime that should be started in her/him? Note that drug resistance was suspected in the HIV patient.
All of the following statements about 'yaws' are true, except:
All of the following are features of mumps, except:
A 2 month old baby presented with acute icteric viral hepatitis. The mother is a known hepatitis B carrier. Mother's hepatitis B virus serological profile is MOST likely to be:
In generalized tetanus, how do toxins typically enter the body?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app