
Infectious Diseases — MCQs

On this page
What is the drug of choice for diarrhea in AIDS?
All of the following are seen in cerebral malaria, except:
Which of the following infections is least likely to be associated with nephropathies?
All are true about amoebic liver abscess except?
Round worms cause all of the following conditions, except:
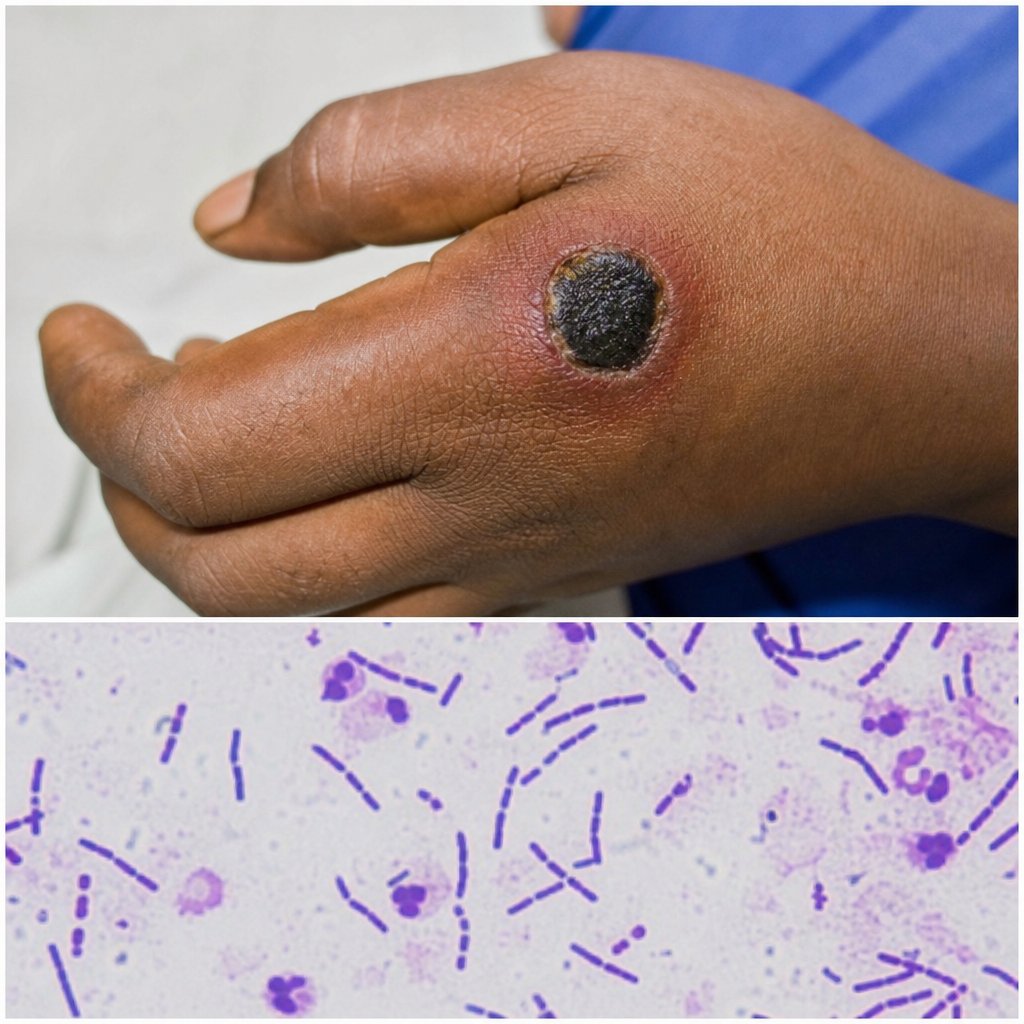
An abattoir worker presented with a lesion on his hand that progressed to form an ulcer. A smear was taken from the ulcer and sent to the laboratory for investigation. What is the diagnosis?
A patient from Himachal Pradesh presents with fever for 5 days, altered sensorium, increased jugular venous pressure, maculopapular rash, and erythema on the back with black necrotic tissue. What is the most appropriate treatment option?
Which of the following is not a common complication of tubercular meningitis?
A febrile 23-year-old college student presents with fatigue and difficulty swallowing. Physical examination reveals exudative tonsillitis, palatal petechiae, cervical lymphadenopathy, and tender hepatosplenomegaly. A complete blood count shows mild anemia, lymphocytosis with approximately 30% of the lymphocytes exhibiting atypical features, and mild thrombocytopenia. The Coombs' test is positive. Which of the following is the most likely complication of this syndrome?
Amoebic liver abscess most commonly affects which part of the liver?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app