
Infectious Diseases — MCQs

On this page
A truck driver, who is HIV-positive, presented with a history of fever since four weeks, and a dry cough, as well as a history of weight loss of about 10 kg. X-ray shows bilateral reticulonodular infiltrates. The most likely diagnosis is:
A 50-year-old HIV-seropositive male presented to the emergency room with multiple episodes of generalized tonic-clonic seizures. The patient is not on highly active antiretroviral therapy. The CD4 count was 45/μL. On examination, the patient was mildly arousable and disoriented, with no nuchal rigidity or focal neurological deficits. Gadolinium-enhanced magnetic resonance imaging and magnetic resonance spectroscopy were conducted. Which is the most appropriate drug to be given in this condition?
Intestinal perforation in typhoid occurs commonly in which part of the intestine?
Kaposi's sarcoma (KS) usually occurs when CD4+ lymphocyte counts are what?
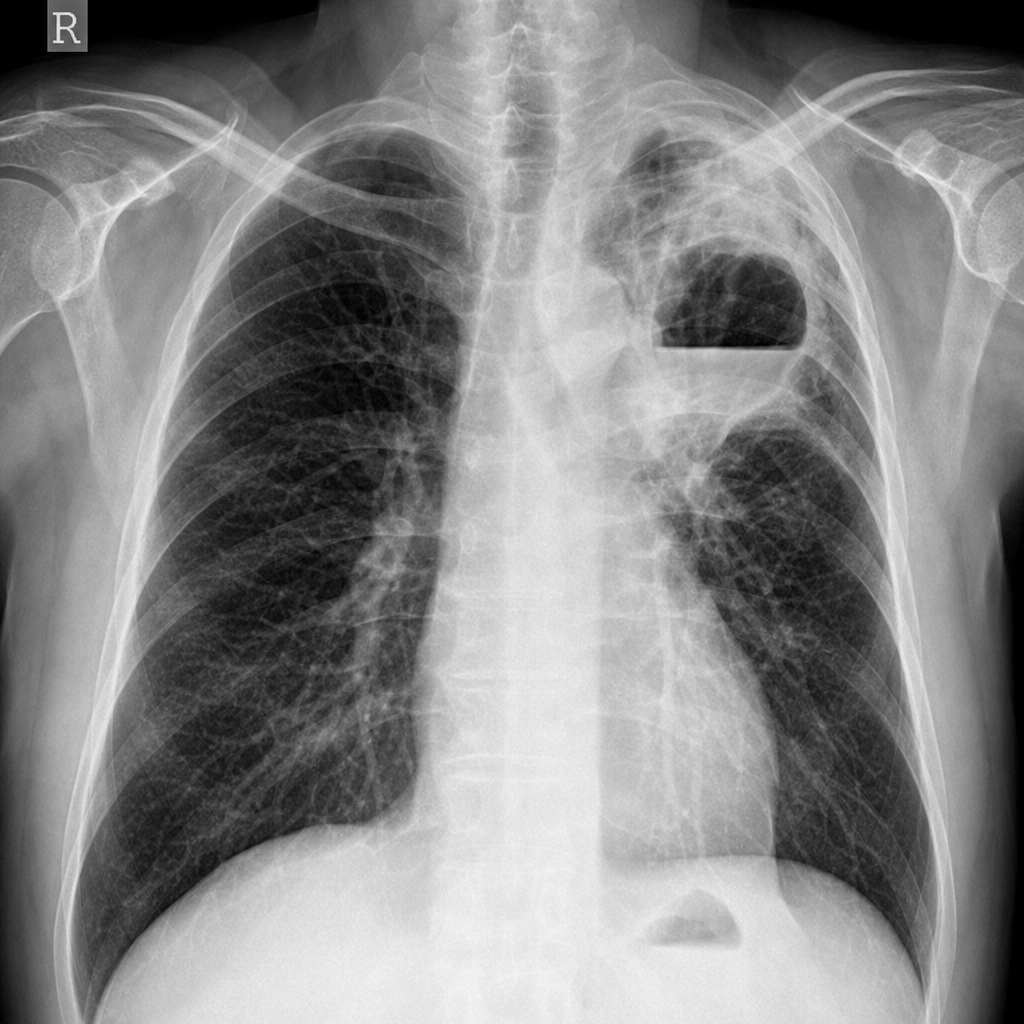
A 63-year-old man with small cell carcinoma of the left mainstem bronchus begins chemotherapy. During the treatment period, he becomes febrile and develops a productive cough. The temperature is 38.7°C (103°F), respirations are 32 per minute, and blood pressure is 125/85 mm Hg. A complete blood count shows leukocytosis (WBC = 18,500/mL). The patient's cough worsens, and he begins expectorating large amounts of foul-smelling sputum. A chest X-ray shows a distinct cavity with an air/fluid level distal to the tumor area. Which of the following is the most likely diagnosis?
What is the route of administration for the tuberculin test?
Which of the following is the most accurate description of thrush?
Tropical splenomegaly is characterized by all the following, except which one?
Manifestation of erythema nodosum leprosum (ENL) include all of the following except:
Which of the following agents is least likely to cause meningitis in the elderly?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app