
Infectious Diseases — MCQs

On this page
A young male admitted for pneumonia for 5 days develops gripping abdominal pain and loose stools. Which drug(s) might be beneficial in managing these new symptoms?
A 30-year-old patient presented with a 30-day history of jaundice. Liver function tests showed a bilirubin of 100mg/dL, SGOT/SGPT of 100/1450, and serum alkaline phosphatase of 240 IU. The patient was positive for HBsAg. What is the confirmatory test to establish acute Hepatitis B infection?
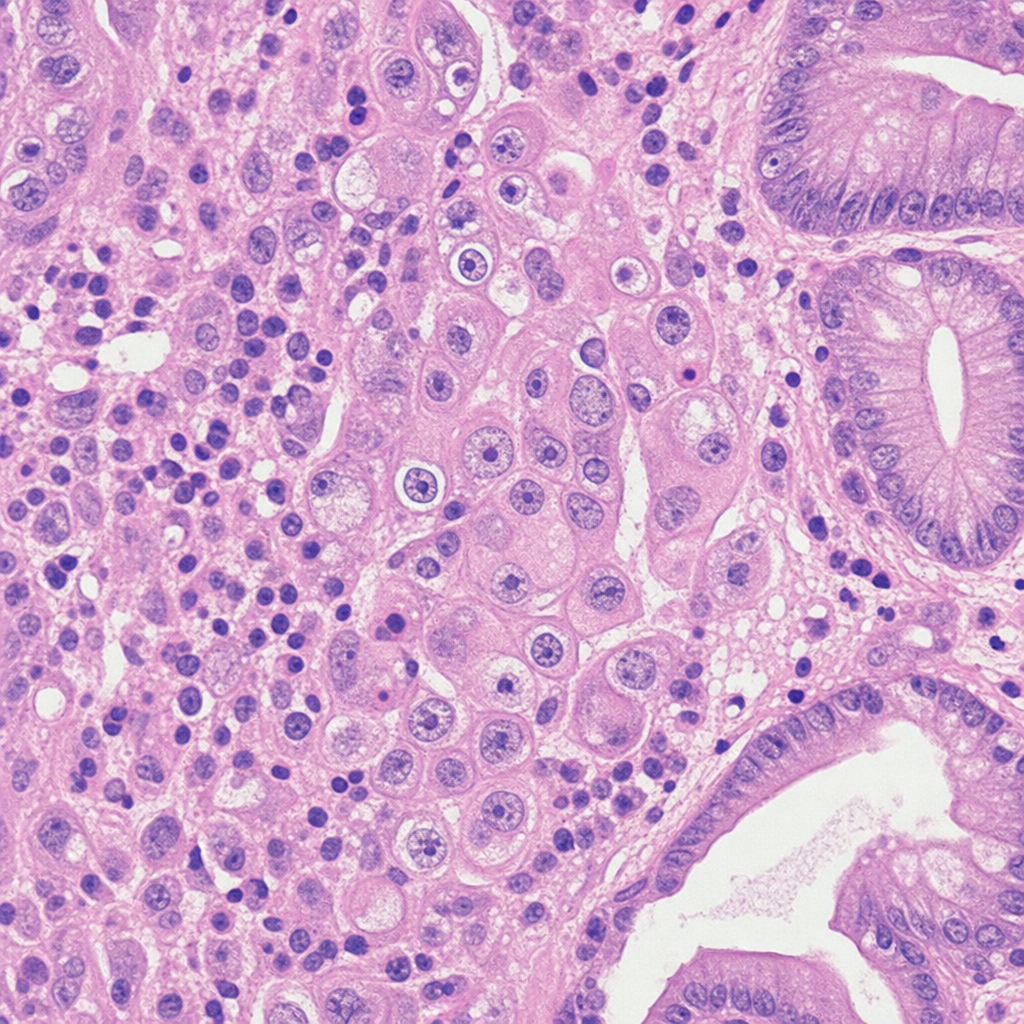
A patient infected with HIV presents with a "Pizza Pie Appearance" on fundoscopy and dysphagia. An upper GI endoscopy biopsy specimen from this patient shows the following. What is the likely diagnosis?
A resident doctor sustained a needle stick injury while sampling blood from an HIV-positive patient. A decision is made to offer the doctor post-exposure prophylaxis. Which one of the following would be the best recommendation?
Which of the following is NOT included in the diagnostic criteria for AIDS?
What is the empirical antibiotic treatment for a suspected case of pneumonia in an outpatient who has not received antibiotics in the past three months?
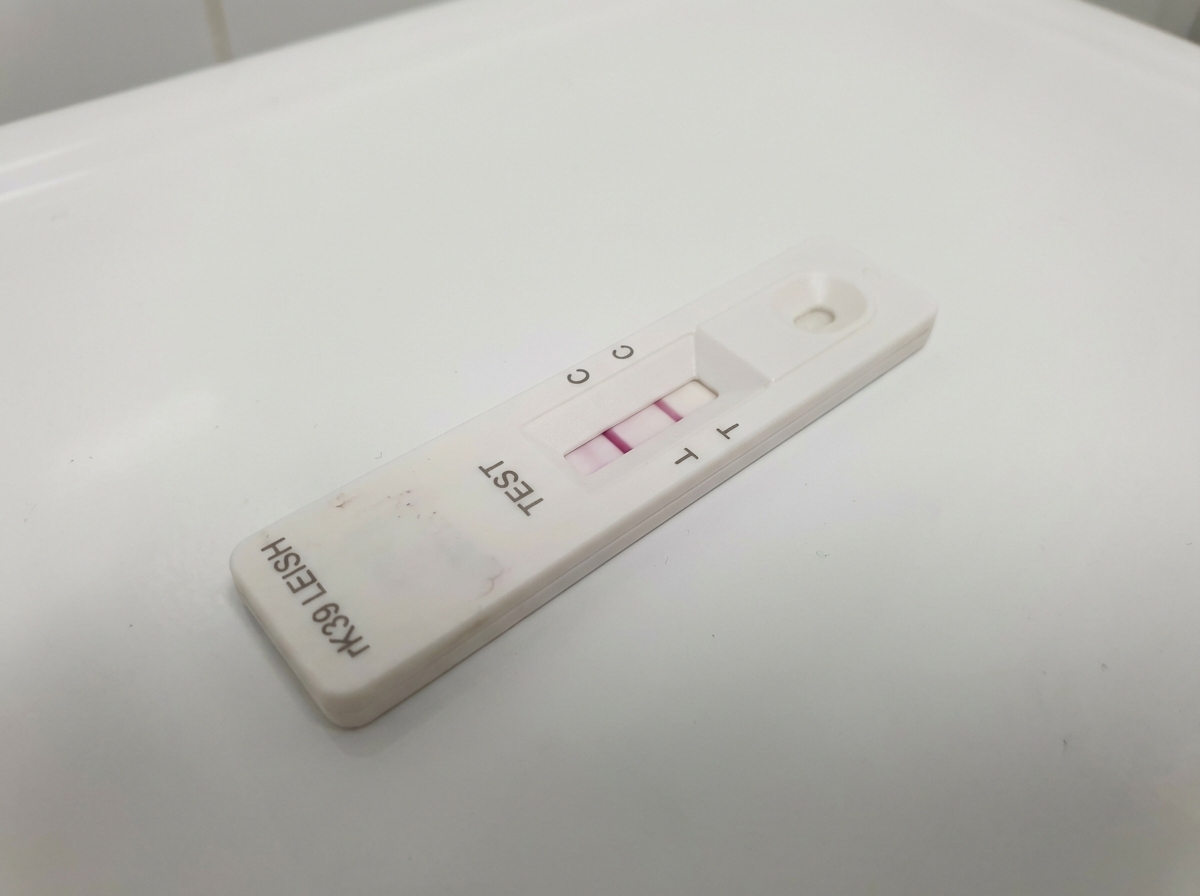
A patient presenting with prolonged fever, splenomegaly, cytopenias and weight loss, with residence in an endemic area and no previously treated visceral leishmaniasis, has an rK39 dipstick kit that was found to be positive. What is the treatment of choice?
A farmer from Central Asia presents with an acute onset of swinging pyrexia, rigor, sweating, and monoarticular arthritis of the hip. He also complained of headache and insomnia. On examination, he is found to have small firm splenomegaly and hepatomegaly. His counts showed leucopenia with relative lymphocytosis. What is the most likely diagnosis?
In the management of complications of falciparum malaria, which of the following is generally avoided?
Which type of cell is present in large numbers in the peritoneal fluid of patients with tuberculous peritonitis?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app