
Infectious Diseases — MCQs

On this page
Most common presentation of extra- pulmonary TB
Which of these is least effective for the treatment of typhoid?
Which type of pulmonary TB is most likely to give sputum positive ?
A 17 years old female presents with sore throat and lymphadenopathy. A diagnostic test reveals the presence of heterophile antibodies. Diagnosis is?
A young male came to the hospital with a clean-cut wound without any bleeding. The patient received a full course of tetanus vaccination 10 years ago. What is the best management for this patient?
A patient diagnosed to be HIV-positive was started on highly active antiretroviral therapy (HAART). Which of the following can be used to monitor treatment efficacy?
A bronchial asthma patient on inhalational steroids presented with white patchy lesions on the tongue and buccal mucosa. What condition is likely to be present in this patient?
A patient hailing from Delhi presents with fever, arthralgia, and extensive petechial rash for 3 days. Lab investigations revealed a hemoglobin of 9 g/ dL, a white blood cell count of 9000 cells/mm3, a platelet count of 20000 cells/mm3, and a prolonged bleeding time. The clotting time was normal. What is the most likely diagnosis?
Punched out ulcers in the esophagus are most commonly associated with which of the following conditions?
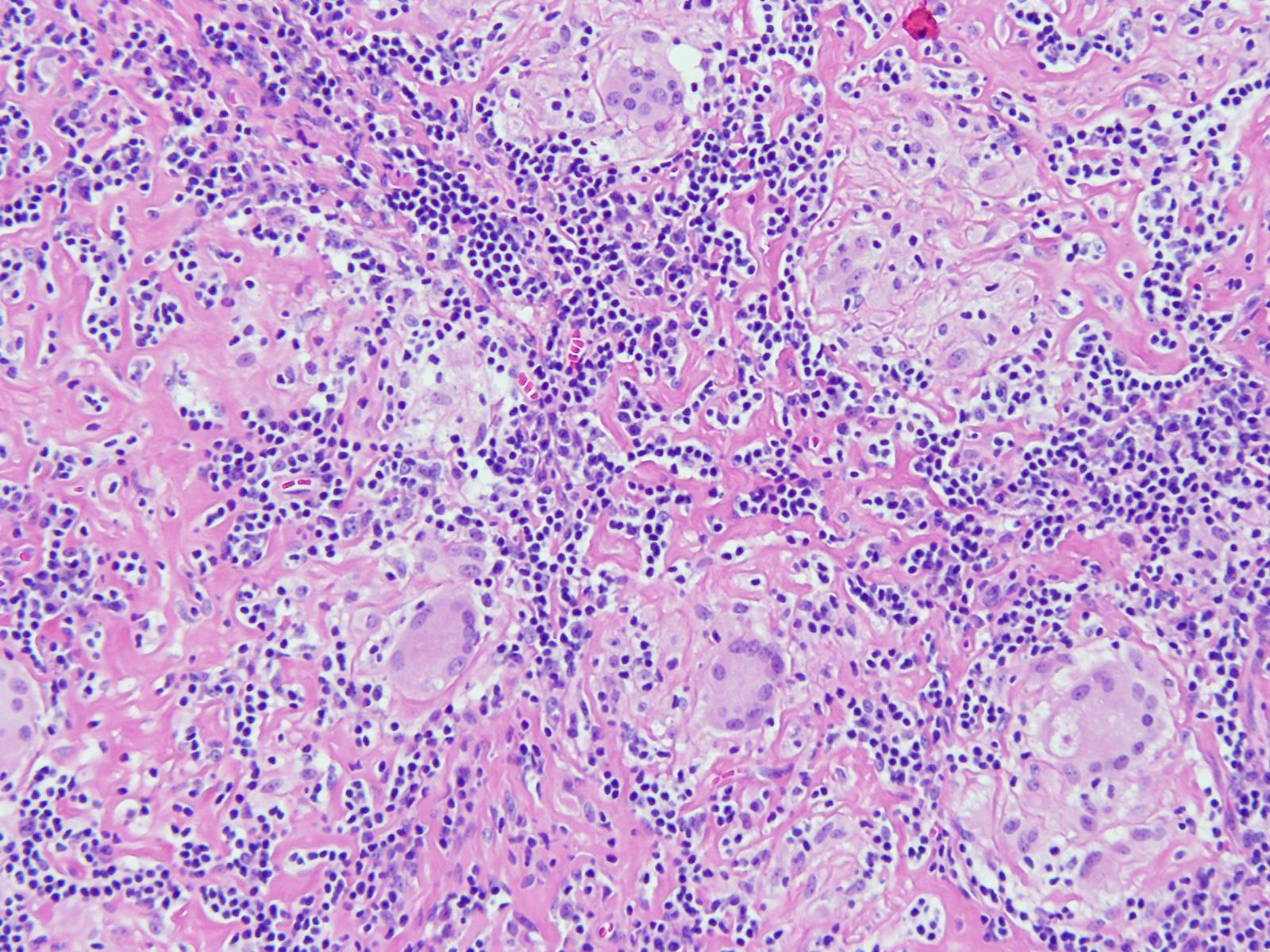
An 11-year-old boy presented with a cough for 15 days. On examination, he was found to have cervical lymphadenopathy. Lymph node biopsy showed the following findings, and acid-fast staining was positive for acid-fast bacilli. What could be the diagnosis?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app