
Infectious Diseases — MCQs

On this page
A 50-year-old farmer presents with cough, fever, and weight loss. CXR shows upper lobe cavitary lesions. Sputum culture reveals acid-fast bacilli resistant to isoniazid and rifampin. What is the next best drug?
A 45-year-old male presents with fever, cough, and cavitary lesion on CXR. What is the most likely diagnosis?
A 45-year-old HIV-positive man presents with fever and cough. Sputum culture shows acid-fast bacilli. Which of the following drugs is essential in the treatment regimen?
A 40-year-old patient presents with frequent watery diarrhea after a recent course of antibiotics. Stool toxin assay is positive for Clostridium difficile. What is the most appropriate treatment?
A 30-year-old patient presents with a dry cough, fever, and myalgia. He recently returned from a household where several family members tested positive for influenza. Chest X-ray shows bilateral ground-glass opacities. What is the most likely diagnosis?
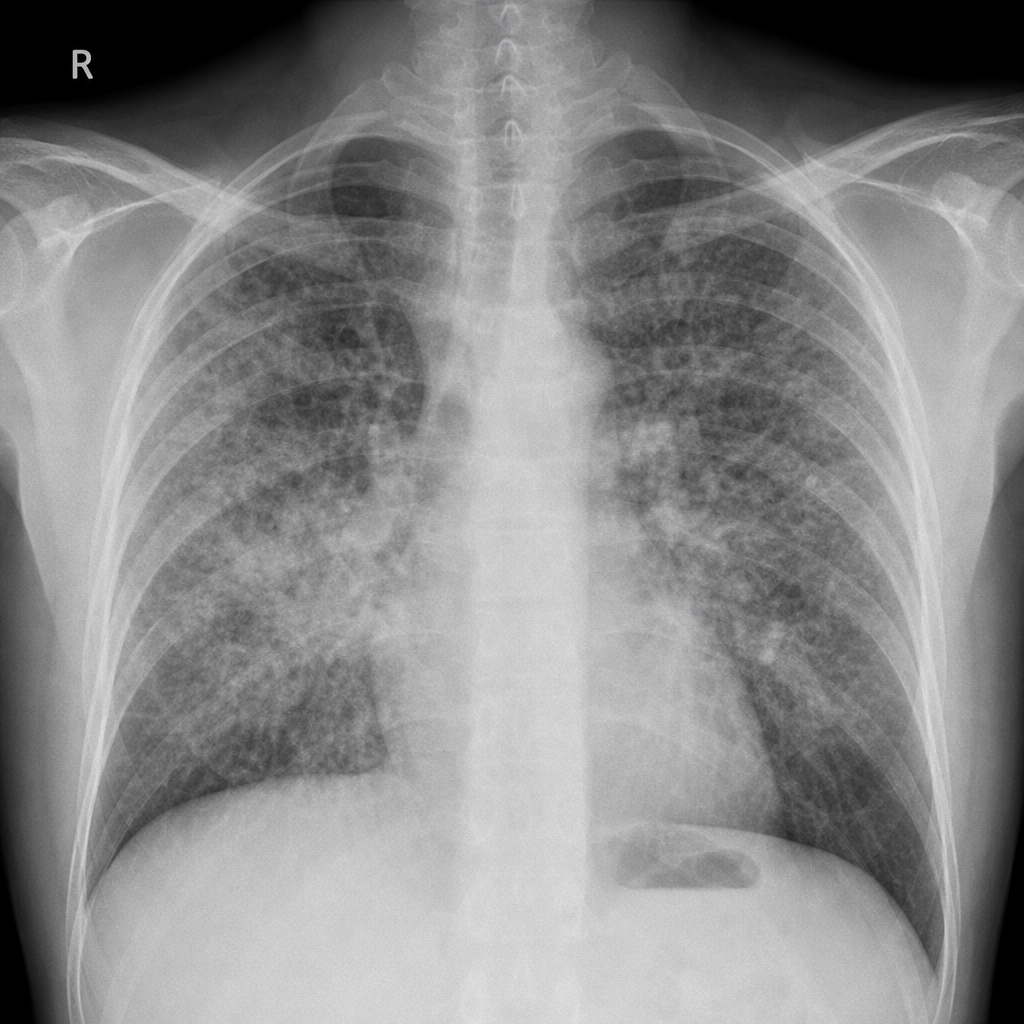
A patient presents with hemoptysis, weight loss, and fatigue. Chest X-ray shows cavitary lesions in the upper lobes. What is the most likely diagnosis?
A 35-year-old woman presents with facial pain, nasal congestion, and purulent nasal discharge for 10 days. What is the most likely diagnosis?
A 25-year-old woman presents with a sudden onset of high fever, chills, and rigors. Blood cultures are pending. What is the next appropriate step in her management?
A 35-year-old male presents with fever, night sweats, and unintentional weight loss over the past 3 months. He has a history of intravenous drug use. Most appropriate next step in the diagnosis?
Which of the following diseases does not typically present with fever, rash, and lymphadenopathy?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app