
Infectious Diseases — MCQs

On this page
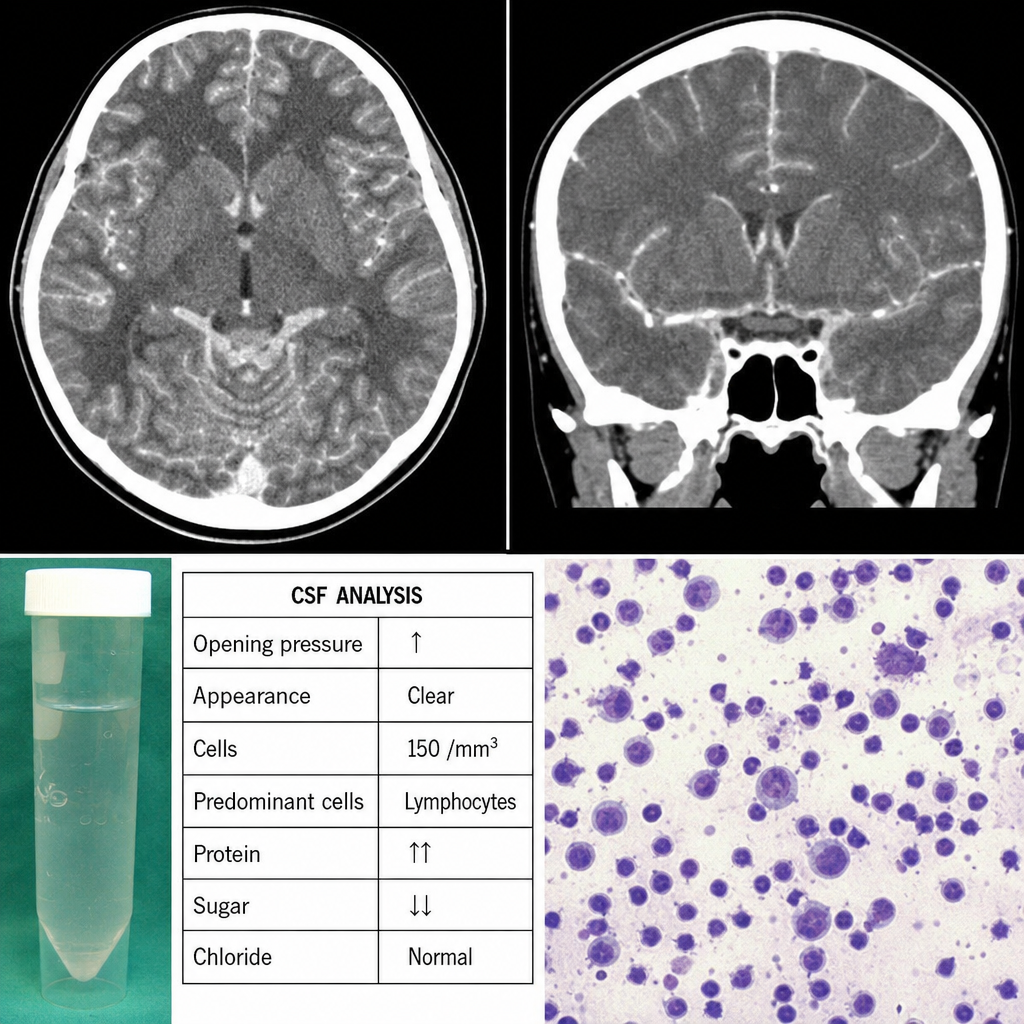
A 17-year-old female presents with a history of fever and headache and now develops altered sensorium. CT scan shows basal exudates with meningeal enhancement. The CSF is most likely to show:
All of the following are strongly associated with AIDS except:
What is the most common extra-intestinal complication of Shigellosis?
A lady presented with fever and rashes. She returned from the USA and gives a history of exposure to ticks. Most probable diagnosis is
Most common single cause of pyrexia of unknown origin
Young female with 3 days fever presents with headache, BP 90/60 mmHg, Heart rate of 114/min, and pin point spots developed distal to BP cuff. Most likely organism is:
Early sign of tetanus is locked jaw due to early involvement of:
Early treatment failure in malaria is indicated by all, EXCEPT:
Most common extra pulmonary involvement of TB ?
The classic opportunistic infection in acquired immune deficiency syndrome is:
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app