
Infectious Diseases — MCQs

On this page
A CSF/serum glucose ratio of < 0.4 is highly suggestive of:
The following about leptospirosis is true except?
In tuberculous meningitis, what is NOT seen:
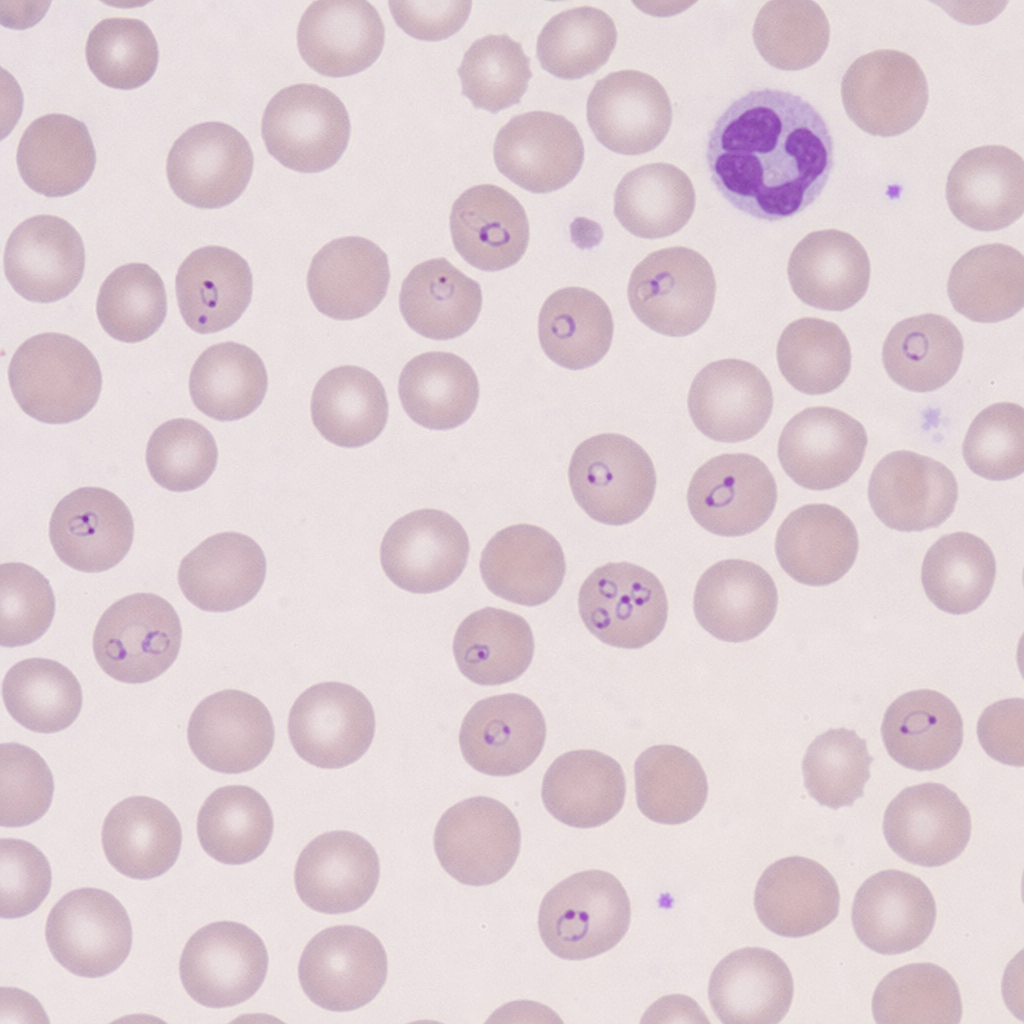
A 34-year-old lady presents with high grade fever with chills and rigors. On examination a firm spleen is felt 3 cm below costal margin with right upper quadrant tenderness. Peripheral smear was prepared. Diagnosis is?
A microbiology laboratory reports growth of Staphylococcus aureus from pus drained from a breast abscess. What is the most likely condition predisposing the patient to the development of a breast abscess?
In bacterial meningitis, CSF has:
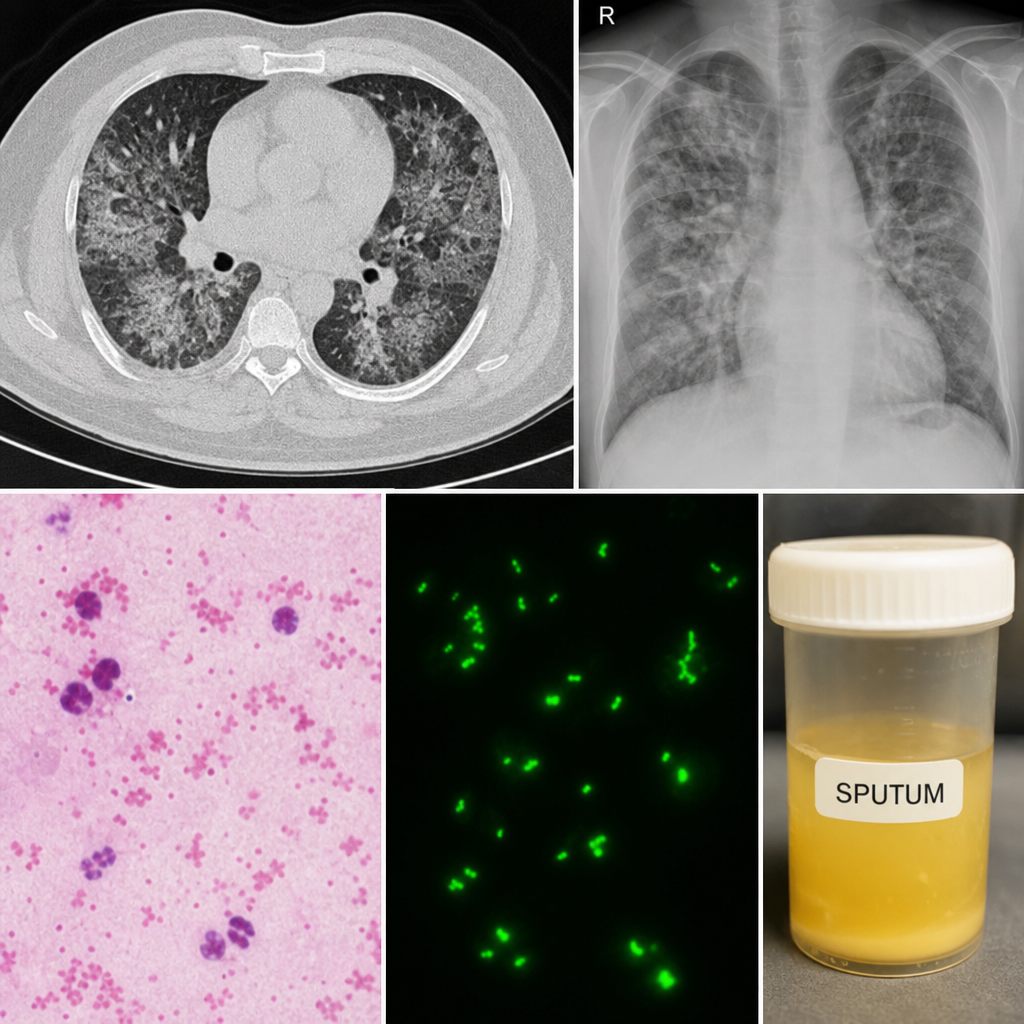
A 40-year-old man presents with fever, productive cough, shortness of breath, mild confusion, and diarrhea. Ten days earlier, he used a shower in a public facility. Sputum Gram stain and direct fluorescent antibody testing are performed, and chest imaging is shown. Which laboratory abnormality is most likely?
Most common muscle involved in Tropical pyomyositis
Six days after receiving several flea bites in a rat-infested shed, a homeless 24-year-old man develops fever, chills, and a rash that spreads from his abdomen to cover his extremities. He is seen at the hospital emergency department, where blood is drawn for analysis. Eight days later, the public health department reports the presence of antibody to one of the rickettsial group antigens. Which of the following is the most likely diagnosis?
Negative Mantoux test is when induration is:
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app