
Infectious Diseases — MCQs

On this page
What is the most common site of abdominal tuberculosis?
A patient, who is a known case of HIV with a CD4 count of 200 cells/cu.mm, presents with 5 days of cough and high-grade fever without chills and rigors. There is no history of diarrhoea, vomiting, or nuchal rigidity. Chest x-ray is normal. What treatment will you give?
A person presents to the hospital with fever and chills. Fever profile is ordered and is found to be negative for malaria and dengue. Rk39 test is found to be positive. What is the treatment of choice?
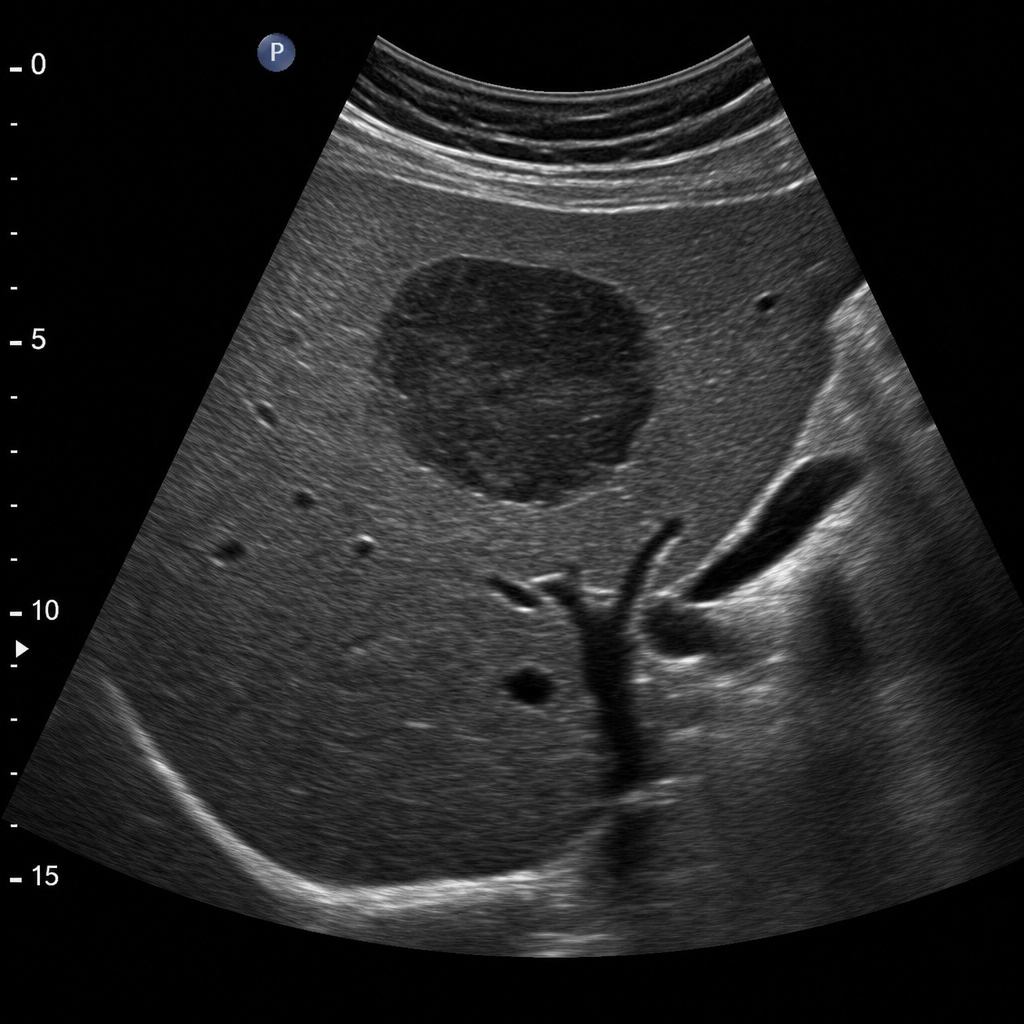
A 35-year-old patient with a history of dysentery for 6 weeks complains of pain in the right upper abdomen. On ultrasound, a hypoechoic hyperdense lesion is seen in the liver. Identify the condition based on the given image?
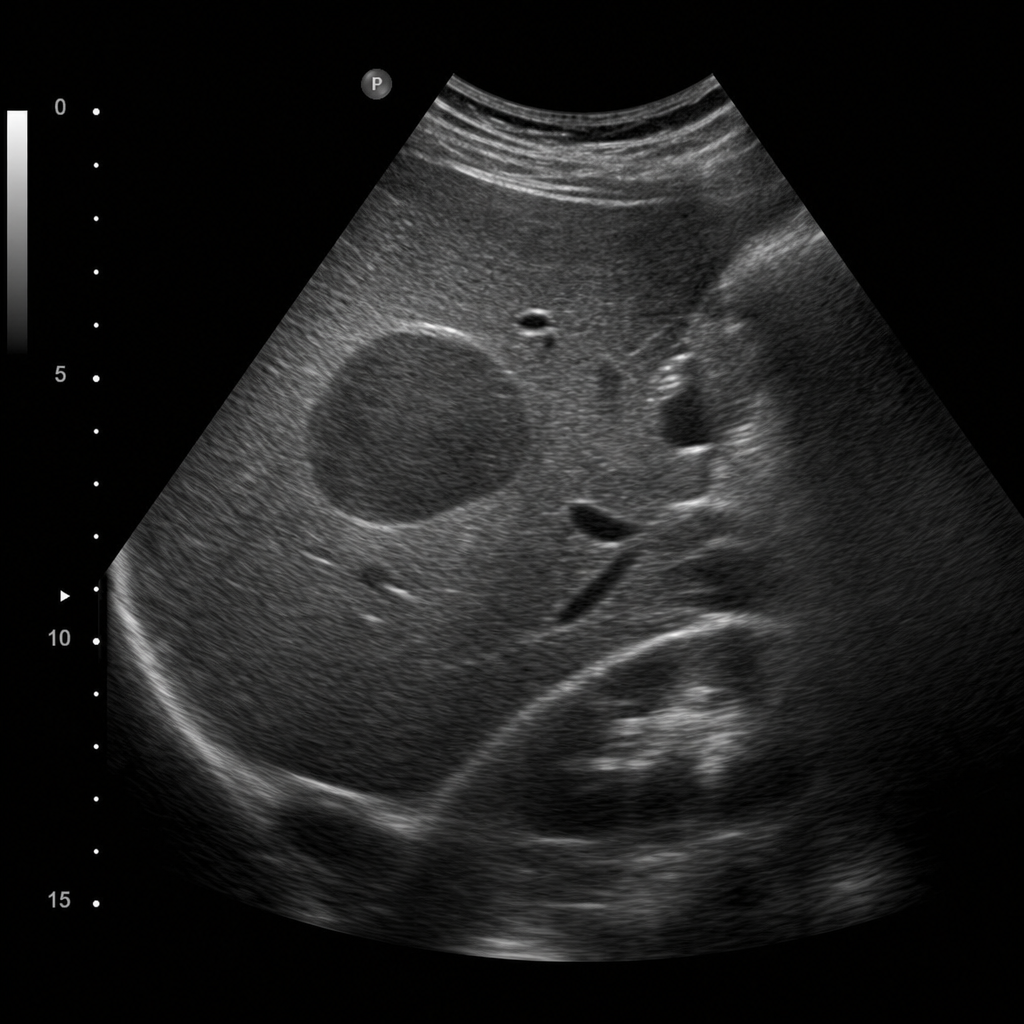
A 35-year-old patient with a history of dysentery for 6 weeks complains of pain in the right upper abdomen. On ultrasound, a hypoechoic hyperdense lesion is seen in the liver. Identify the condition based on the given image?
An ICU patient is suffering from Rhinovirus infection. How do we treat the patient?
During the discharge of a COVID patient treated with steroids and remdesivir, which of the following will you inform him about? 1. Repeat RT-PCR after 7 days of discharge 2. Watch for the persistence of Anosmia 3. Watch for headache and nasal discharge 4. Monitor glucose levels 5. Watch for Sinusitis symptoms
A forest officer develops the lesion as shown in the image. Which of the following is not a differential to consider?

In HIV-positive patients with gonorrhea, which of the following statements is TRUE regarding management?
A 42-year-old man with a history of gout and hypertension presents to his family physician with a complaint of increased left knee pain over the past 2 days. He also reports swelling and redness of the left knee and is unable to bear weight on that side. He denies any prior surgery or inciting trauma to the knee. His temperature is 97.0°F (36.1°C), blood pressure is 137/98 mm Hg, pulse is 80/min, respirations are 13/min, and oxygen saturation is 98% on room air. Physical examination reveals a left knee that is erythematous, swollen, warm-to-touch, and extremely tender to palpation and with attempted flexion/extension movement. His left knee range of motion is markedly reduced compared to the contralateral side. Joint aspiration of the left knee is performed with synovial fluid analysis showing turbid fluid with a leukocyte count of 95,000/mm^3, 88% neutrophils, and a low glucose. Gram stain of the synovial fluid is negative. Results from synovial fluid culture are pending. Which of the following is the best treatment regimen for this patient?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app