
Infectious Diseases — MCQs

On this page
WHO defines a multi-drug resistant (MDR) Tuberculosis strain as one that is:
Current WHO recommendations for initiating Antiretroviral treatment (ART) in HIV +ve individuals is:
Cellulitis is:
A pregnant woman in 2nd trimester of pregnancy from North Eastern State has been diagnosed with uncomplicated P. falciparum. She should be treated with:
A 50 year old female presents to the emergency with pain, swelling and redness over the left foot following a trivial trauma 3 days back. On examination, the swelling over the left foot is poorly localised; local tenderness and erythema are present and crepitus is absent; distal pulsations are palpable. The most likely clinical diagnosis is
Which of the following statements is not true regarding HIV infection?
Consider the following features of cholera: 1. Onset with purging. 2. No nausea or retching. 3. No tenesmus. 4. Leukocytosis. Which of the above features of cholera differentiate it from food poisoning?
Tuberculosis in HIV positive individuals is characterized by which of the following? 1. More frequent negative sputum smears. 2. More false–negative tuberculin test results. 3. More extra–pulmonary tuberculosis. 4. More cavitating lesions in lungs as shown by chest X-ray. Select the correct answer using the code given below:
Which of the following is not a clinical feature of tetanus?
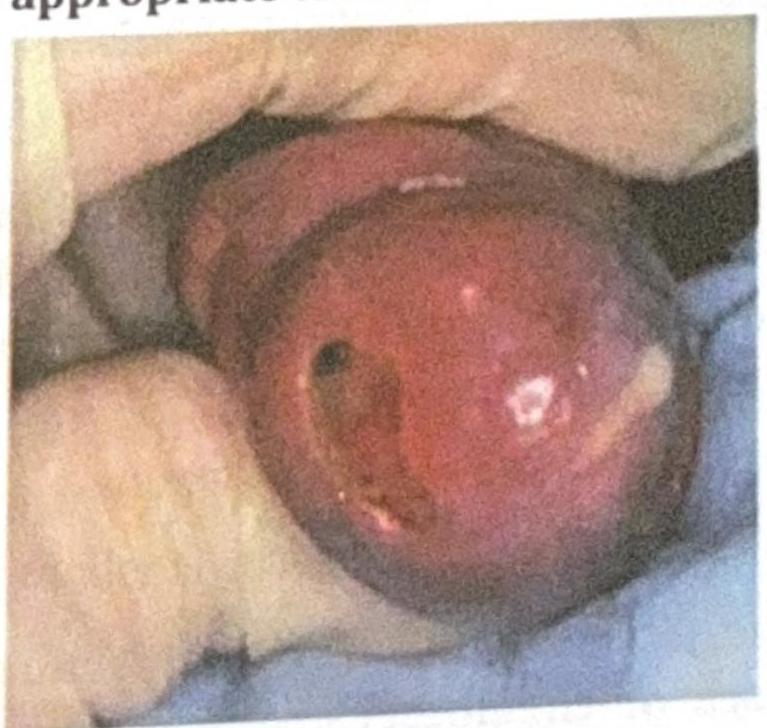
An adult woman presents with the clinical condition shown in the image, and a Gram stain reveals Gram-negative diplococci. What is the most appropriate treatment?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app