
Infectious Diseases — MCQs

On this page
A patient undergone a Solid organ transplant is having the following lesions which are present on oral mucosa and sites shown below. Which of the following is incriminated in causing the same?

Which of the following statements are correct regarding Weil's disease? I. It is caused by a virus named leptospira II. Acute kidney injury can lead to oliguria in this disease III. Microscopic agglutination is the investigation of choice IV. Ceftriaxone given parenterally is effective treatment Select the correct answer using the code given below :
Which one of the following conditions is a complication of bacterial pharyngitis involving extension of infection into the internal jugular veins leading to thrombosis and metastatic dispersal of the organism?
Which of the following statements are correct regarding Mantoux test for tuberculosis? 1. It entails injecting 1 TU (Tuberculin Unit) of PPD (Purified Protein Derivative) in 0.1 mL intradermally. 2. The injection should be given with the needle bevel facing downward. 3. When placed correctly, the injection should produce a pale wheal of the skin, 1 - 2 mm in diameter. 4. The injection should be given with a tuberculin syringe. Select the correct answer using the code given below:
Which one of the following is the commonest extra-salivary gland manifestation of mumps in adults?
Which of the following is NOT a complication of malaria in pregnancy?
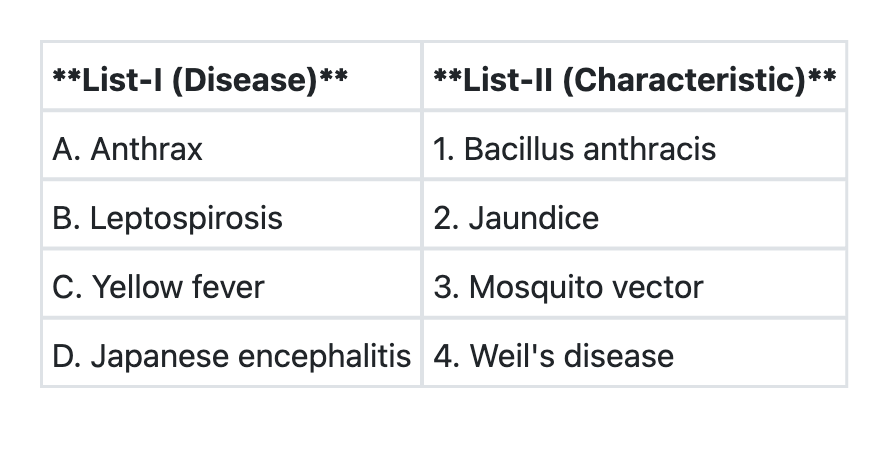
Match List-I with List-II by selecting the MOST DISTINCTIVE association for each disease, and select the correct answer using the code given below the Lists:
The complications of ascaris lumbricoides infestation include all of the following except :
The most common opportunistic infection observed in patients with AIDS is
A recently married woman presents with dysuria and increased urinary frequency of two-days duration. On physical examination, her body temperature is 38°C and her vital signs are normal. Her gynaecologic examination does not reveal any vaginal discharge, vaginitis or cervicitis. Her urine analysis reveals 14 WBC per high power field and many gram negative rods. Which of the following is the most appropriate pharmacotherapy ?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app