
Infectious Diseases — MCQs

On this page
The following cell type is seen in peripheral smear of a patient with membrane over the tonsils. All can be used in treatment except?
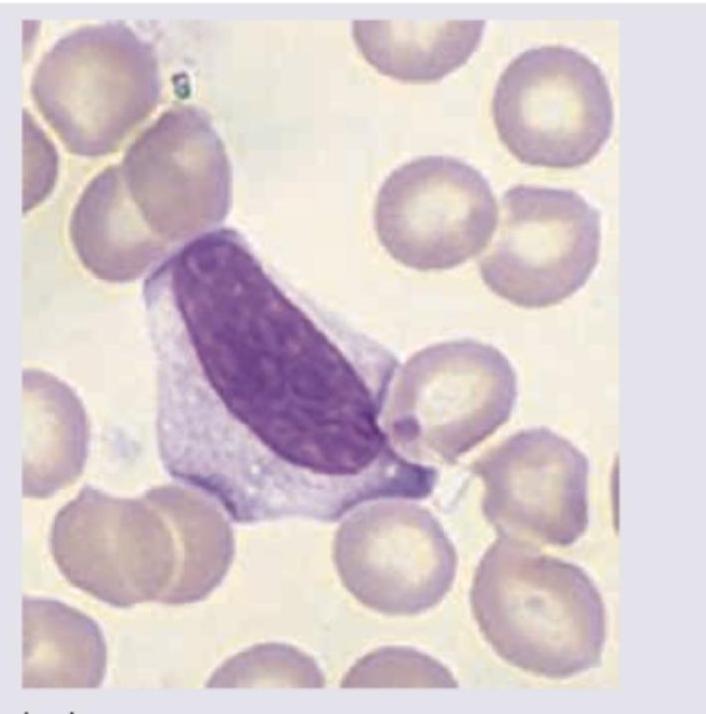
Which of the following will best describe this patient?
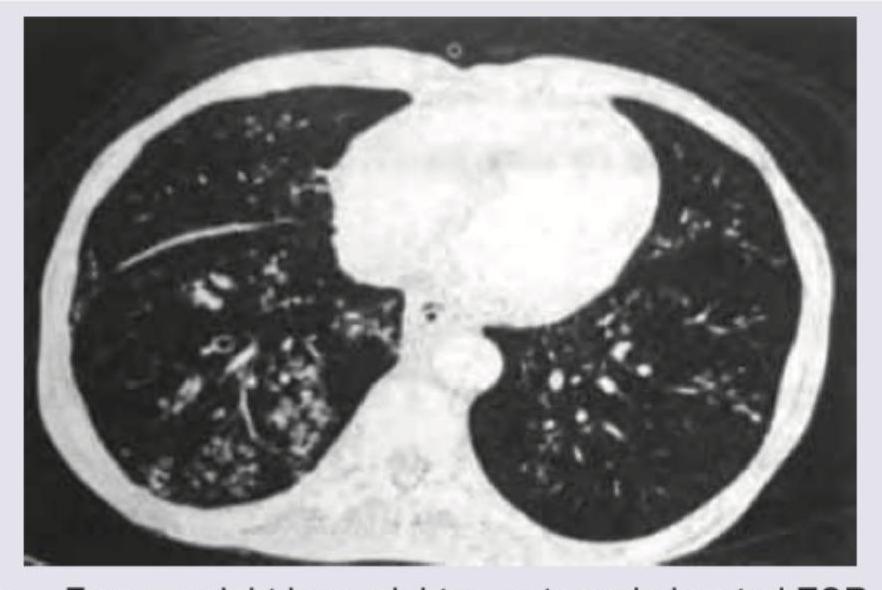
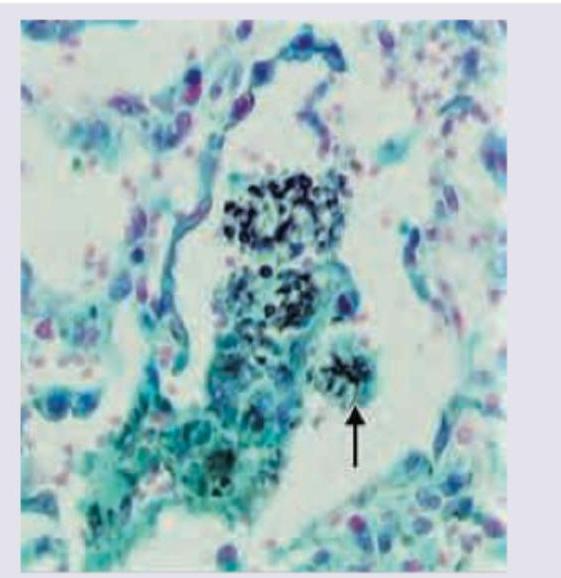
Drug of choice for following infection (as shown in image) in a HIV patient: (NEET Pattern 2019)
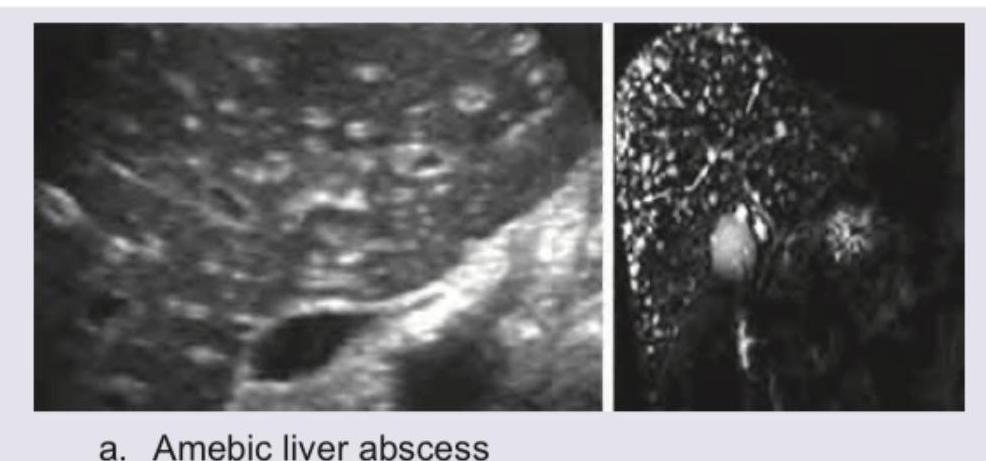
A 28-year-old female patient presents with abdominal pain, fever, night sweats, malaise, and intercostal tenderness. Past history of bloody diarrhea is present. USG liver of the patient is given. Which among the following statements is false?

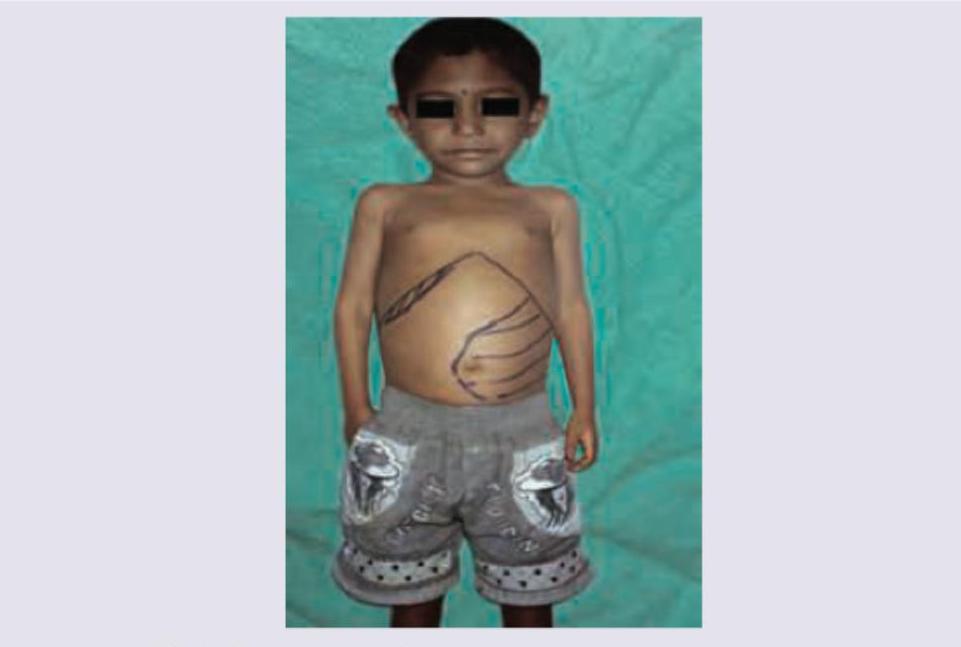
Which of the following infections in most commonly seen in this transfusion dependant child shown below?
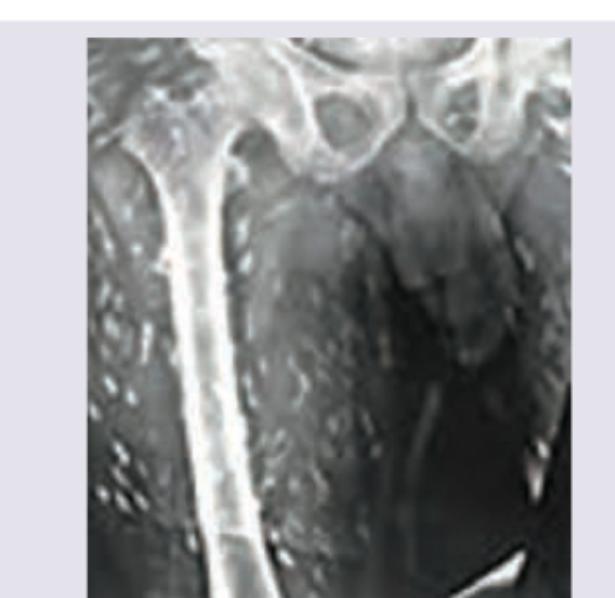
The image shows cigar-shaped soft tissue calcification/rice grain calcification in muscles, which is characteristic of cysticercosis. This finding in a patient with neurocysticercosis is categorized as:
A 48-year-old intravenous drug abuser presents with vomiting, jaundice and right hypochondrium pain. USG abdomen shows presence of:
A 45-year-old alcoholic presents with severe respiratory distress. On examination bronchial breathing was heard in right infraclavicular and inframammary areas. The X-ray chest was performed. The best antibiotic to be given to the patient is:

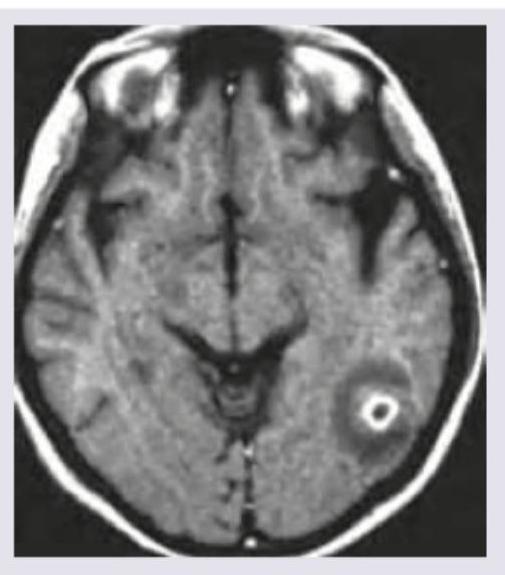
A 30-year-old patient has suffered from multiple episodes of GTCS for the last one week. MRI was performed. All are true about the condition except:
The finding shown below is used for diagnosis of CNS parasitic lesion. Which of the following best describes the condition?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app