
Infectious Diseases — MCQs

On this page
CSF examination of a patient shows high protein, markedly low sugar, low chloride, and increased neutrophils. What is the most likely diagnosis?
Corticosteroids are absolutely contraindicated in which of the following types of tuberculosis?
All of the following are indications for steroid use in Tuberculosis except?
A young patient presents with fever and right upper quadrant pain. Clinical examination reveals hepatomegaly but no jaundice. Ultrasound reveals a solitary, homogeneous, hypoechoic lesion in the right lobe measuring 5 cm x 5 cm x 4 cm. Tests for hydatid disease were negative. Which of the following is the best recommendation for initial treatment?
A 17-year-old man presents with fatigue, malaise, fever, and sore throat. He has no significant past medical history and is not on any medications. Physical examination reveals enlarged, palpable cervical lymph nodes. He reports no weight loss or night sweats. Laboratory investigations include a normal chest x-ray, negative throat swab, and an abnormal blood film with atypical lymphocytes. His hemoglobin is 15.5 g/dL; hematocrit 42%; platelets 290,000/mL; WBC 10,500/mL, with 45% segmented neutrophils, 1% eosinophils, and 54% lymphocytes, of which 36% were atypical. Which of the following is the most appropriate initial diagnostic test?
Which of the following is NOT a feature of cerebral malaria?
All are features of tabes dorsalis, except?
CMV retinitis in HIV occurs when the CD4 counts fall below which of the following levels?
What is the drug of choice for the treatment of latent syphilis?
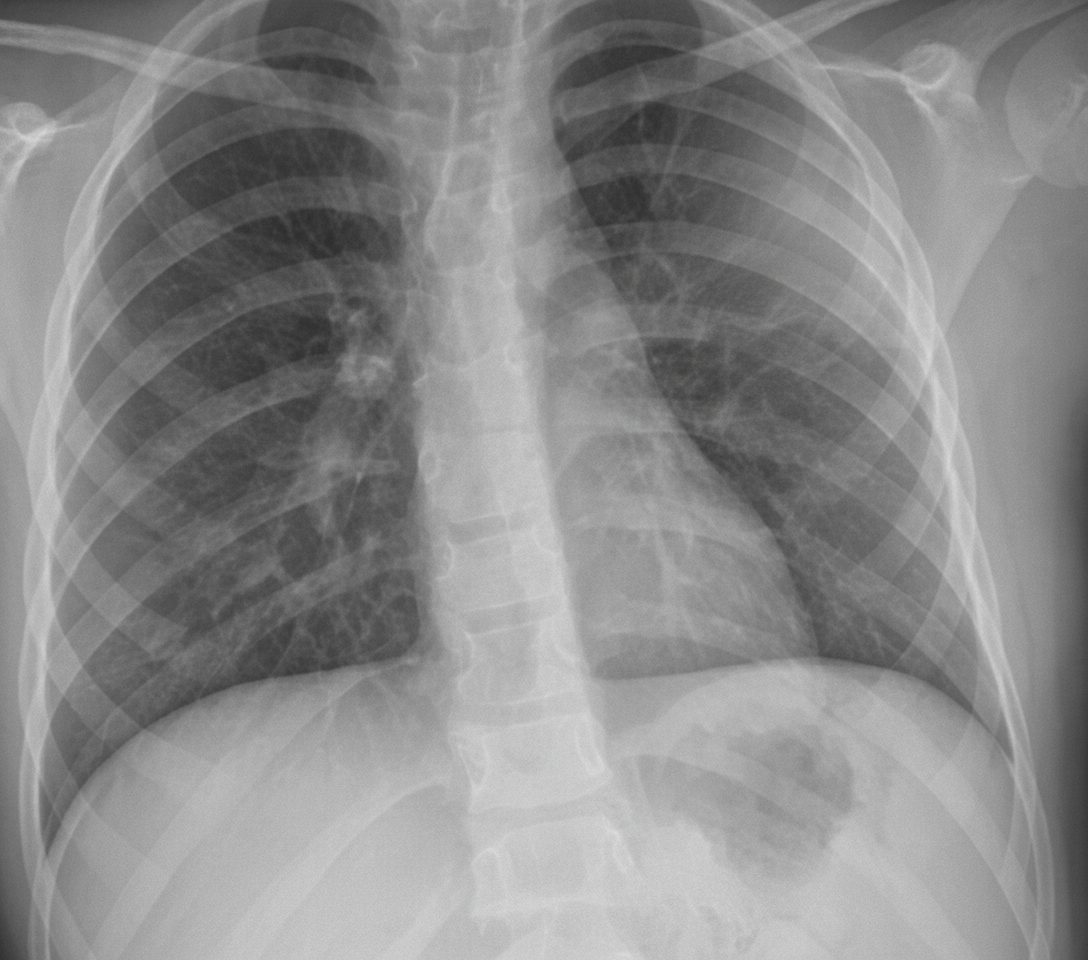
A 54-year-old non-smoking male presents with a flulike illness. Initially treated symptomatically, he returns two days later still feeling unwell. His primary physician prescribes a macrolide along with symptomatic treatment. After five days, the patient reports persistent fever, increasing fatigue, weakness, and cough. He also experiences pain and limited motion in his right wrist, and left groin pain with difficulty ambulating. On physical exam, vital signs include pulse 110 bpm, temperature 102°F, respirations 24/min, and blood pressure 100/68 mm Hg. He appears weak and has lost 8 lb in 10 days. Lung examination reveals egophony and E to A changes in the left anterior and posterior fields. Physical findings include swelling with skin sloughing on the right wrist and tenderness with limited movement in the left groin. Laboratory data shows Hb 11 g/dL, Hct 33%, WBCs 16,000/uL with 90% neutrophils, BUN 42 mg/dL, creatinine 1.1 mg/dL, sodium 142 mEq/L, and potassium 3.4 mEq/L. Arterial blood gases on room air are: pH 7.45, PCO2 34 mm Hg, PO2 65 mm Hg. A chest X-ray is provided. Associated findings may include all of the following except?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app