
Infectious Diseases — MCQs

On this page
Serology of a young man shows HBsAg, but HBeAg is negative with normal levels of AST and ALT. He is asymptomatic. What is the next line of management?
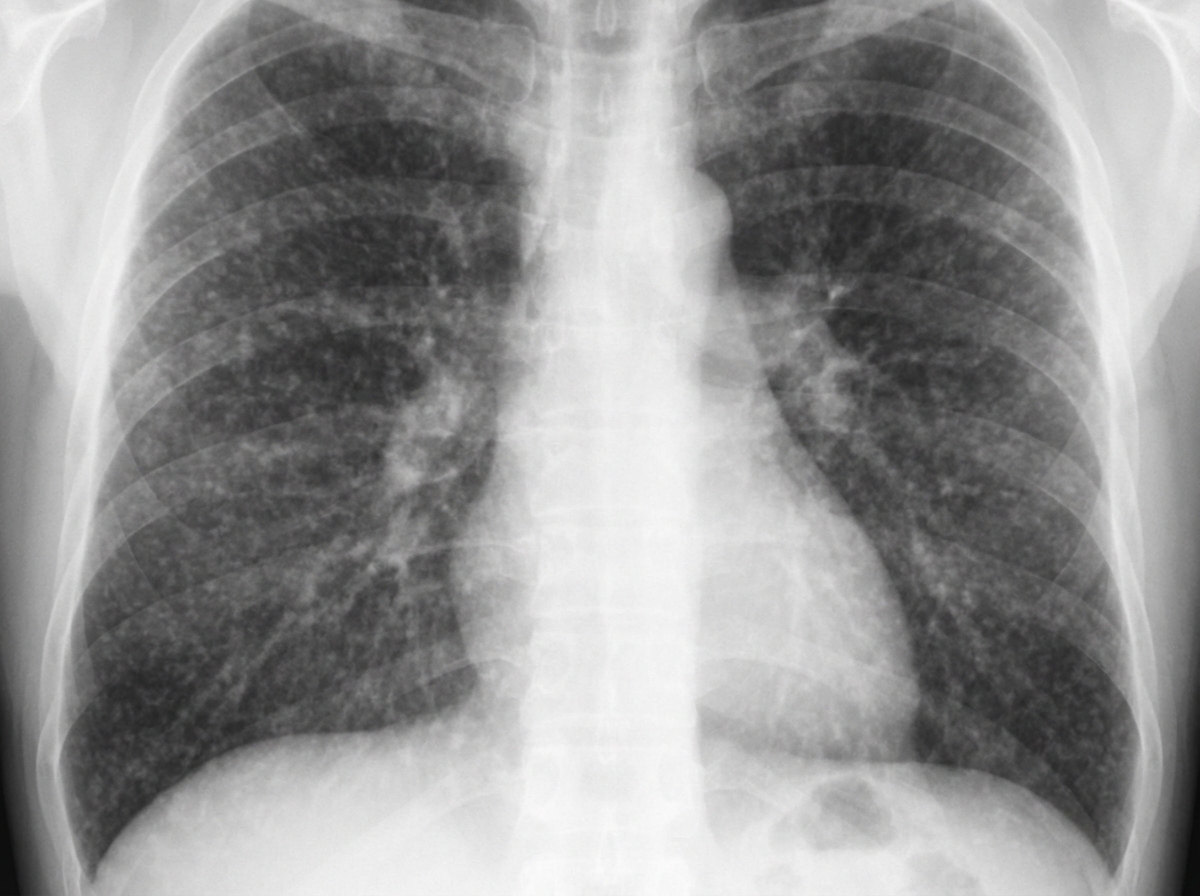
A 71-year-old man presents with low-grade fever, generalized malaise, and a feeling of being run-down. He has experienced weight loss and exhibits stigmata of chronic illness. There is no history of occupational exposure. On physical examination, vital signs are: pulse 110 bpm; temperature 99°F; respirations 19/min; blood pressure 90/60 mm Hg. The patient is frail and appears cachectic with temporal wasting. Other aspects of his physical exam are unremarkable. Laboratory data: Hb 10 g/dL; Hct 30%; MCV 90 fL; WBCs 3000/uL; differential normal; BUN 19 mg/dL; creatinine 1.0 mg/dL; sodium 129 mEq/L; potassium 5.0 mEq/L; ABGs (RA): pH 7.42, PCO2 35 mm Hg, PO2 58 mm Hg. Spirometry: FVC 60% of predicted; FEV1 60% of predicted. PPD skin test is negative (0 mm); induced sputum for AFB smear is negative. Chest radiograph is shown. What is the most likely diagnosis?
Which of the following is NOT a feature of dengue hemorrhagic fever?
Which of the following statements about cysticercosis is true?
What is the increased risk factor for developing tuberculosis (TB) in a patient with a positive Mantoux test?
A patient with an 8 cm x 8 cm abscess in the right lobe of the liver was treated with multiple aspirations and systemic amebicide. A cavity remains in the right lobe, which is now empty. A seven-day course of luminal amebicides has been completed. What is the recommended follow-up plan?
A young butcher cuts his forearm with a knife. Over the next week, he notices swelling, redness, and warmth at the site. Four days later, he presents to the emergency department with fever, shaking chills, and severe lower back pain. Physical examination reveals a temperature of 39.4 C (102.9 F), swelling in his forearm with an area of central softness, and tenderness to pressure over his lower spine. Laboratory data show a leukocyte count of 14,000/mm3 with 81% polymorphonuclear leukocytes. Blood cultures grew a gram-positive cocci in clusters on blood agar; colonies show a yellow pigment, and the organism is positive on mannitol/salt agar. The organism is catalase and coagulase positive. Which of the following is the most likely pathogen?
Which of the following is NOT seen in acute HIV syndrome?
Which of the following is NOT essential when managing a febrile neutropenic patient?
Fulminant Hepatitis E is typically seen in which demographic group?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app