
Infectious Diseases — MCQs

On this page
Waterhouse-Friderichsen syndrome is caused by which organism?
A 19-year-old male presents with a 1-week history of malaise and anorexia followed by fever and sore throat. On physical examination, the throat is inflamed without exudate, and there are a few palatal petechiae. Cervical adenopathy is present. The liver is percussed at 12 cm and the spleen is palpable. Throat cultures are negative for group A streptococci, and peripheral blood smears show atypical lymphocytosis. Laboratory findings include: Hb: 12 g/dL, Reticulocytes: 4%, WBC: 14,000/uL with 60% Lymphocytes, Total Bilirubin: 2.0 mg/dL, LDH: 260 IU/L, AST: 40 U/L, and ALT: 35 U/L. What is the next best investigation?
Occurrence of diplopia, dysphagia, dysarthria, blurring of vision, and muscle weakness could be due to which of the following?
A 35-year-old woman presents with a 2-day history of burning on urination. Urinalysis shows marked positivity for leukocyte esterase but no reactivity for nitrite. Urine culture grows a large number of organisms. Which of the following bacteria is most likely responsible for this patient's infection?
Pulmonary tuberculosis is more common in the following associated diseases, except:
A 20-year-old woman presents with a 2-week history of fever, malaise, and brown-colored urine. She recently visited Mexico. Physical examination reveals jaundice, mild hepatomegaly, and tenderness in the right upper quadrant. The serum bilirubin is 7.8 mg/dL, with 60% in the conjugated form. Serum levels of AST and ALT are markedly elevated (400 and 392 U/L, respectively). Serum albumin and immunoglobulin levels are normal. Serum IgM anti-hepatitis A virus (anti-HAV) is positive. IgG anti-hepatitis B surface antigen (anti-HBsAg) antibodies are positive. Anti-hepatitis C virus antibodies are negative. What is the most likely diagnosis?
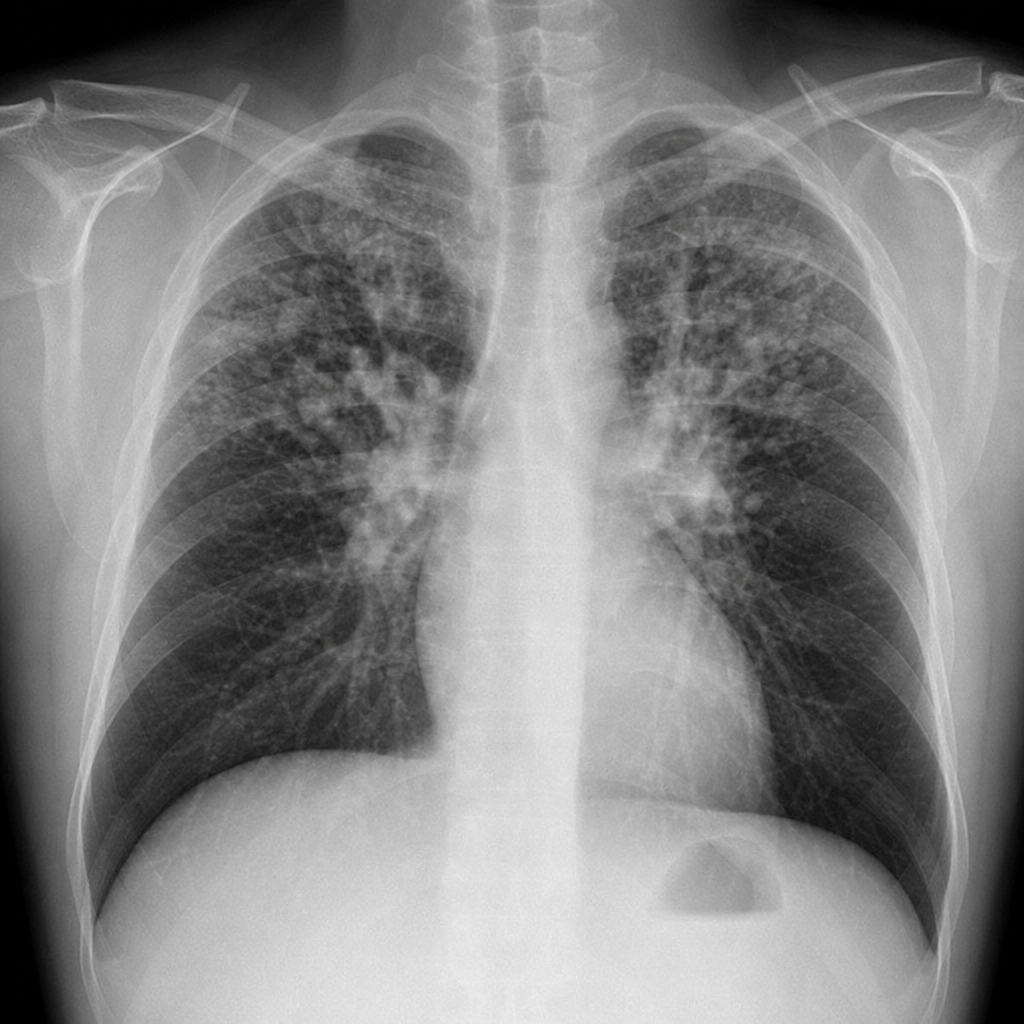
What is the most likely diagnosis in this patient with cough?
What is the treatment of choice for a patient with meningococcal meningitis who is allergic to penicillin?
An 18-year-old male presented with acute onset descending paralysis after 3 days of intake of canned food. There is also a history of blurring of vision for the same duration. On examination, the patient has quadriparesis with areflexia. Both the pupils are nonreactive. What is the most probable diagnosis?
A 19-year-old man presents to the emergency department after being bitten by a stray dog. There is a penetrating wound to the right forearm. The dog could not be found. The wound was cleaned with water and povidone-iodine solution. What is the most appropriate next step in management?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app