
Infectious Diseases — MCQs

On this page
A patient is found to be positive for HBs Ag on routine laboratory evaluation. Other serological tests for hepatitis are unremarkable. He is clinically asymptomatic and liver enzymes are within the normal range. Which of the following best describes his diagnosis?
A 45-year-old female is diagnosed with pneumococcal meningitis. While awaiting culture sensitivity results, what is the best empirical treatment to start?
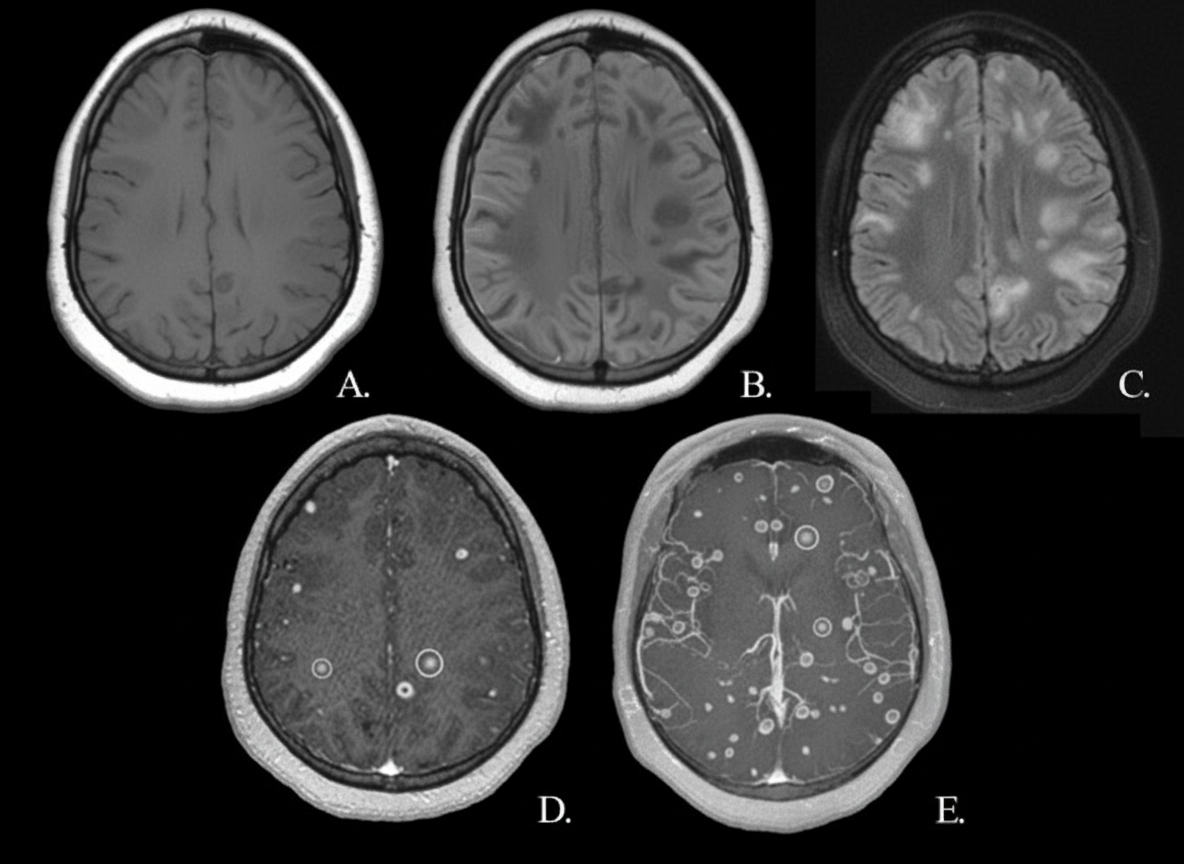
A 30-year-old male presented to the hospital with complaints of seizures. An MRI of the brain was performed, as shown. The imaging reveals multiple viable cystic lesions with ring enhancement and scolex signs. What is the most probable diagnosis and its management, respectively?
Antibiotic prophylaxis is not recommended in which of the following procedures?
Which of the following is NOT an AIDS-defining illness?
What is the diagnosis in a patient who appears sick, has a bull neck, and is tachycardic?
Which of the following has been strongly implicated as a causative agent for Kaposi's sarcoma?
Which of the following is an AIDS-defining opportunistic illness?
What represents a medical emergency in an asplenic patient?
Mulberry molars are characteristic features of which condition?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app