
Infectious Diseases — MCQs

On this page
A 57-year-old male is admitted to the hospital for a suspected kidney infection (likely pyelonephritis). The patient is placed on intravenous antibiotic therapy but continues to have a temperature of 103°F after 3 days of therapy. The urine culture grows lactose-fermenting Gram-negative bacilli which are pan drug-sensitive. On examination, he appears ill and has marked left flank tenderness. Ultrasound depicts a specific finding. What is the most likely diagnosis?

Which one of the following is not a feature of leptospirosis?
A 40-year-old HIV-positive lady presented with multiple, discrete, firm lymphadenopathy in the posterior cervical and supraclavicular regions of 6 months duration. She also complained of chronic cough during this period. A surgical biopsy of the lymph nodes was diagnosed as TB lymphadenitis. Which statement is true in this setting?
Which of the following statements regarding cysticercosis is FALSE?
A 32-year-old male who recently visited a sea coast presented with an ulcer over the left leg. What is the probable causative organism?
What is the most common disease caused by Cytomegalovirus (CMV) in post bone-marrow transplant patients?
What does I.R.L.S. stand for?
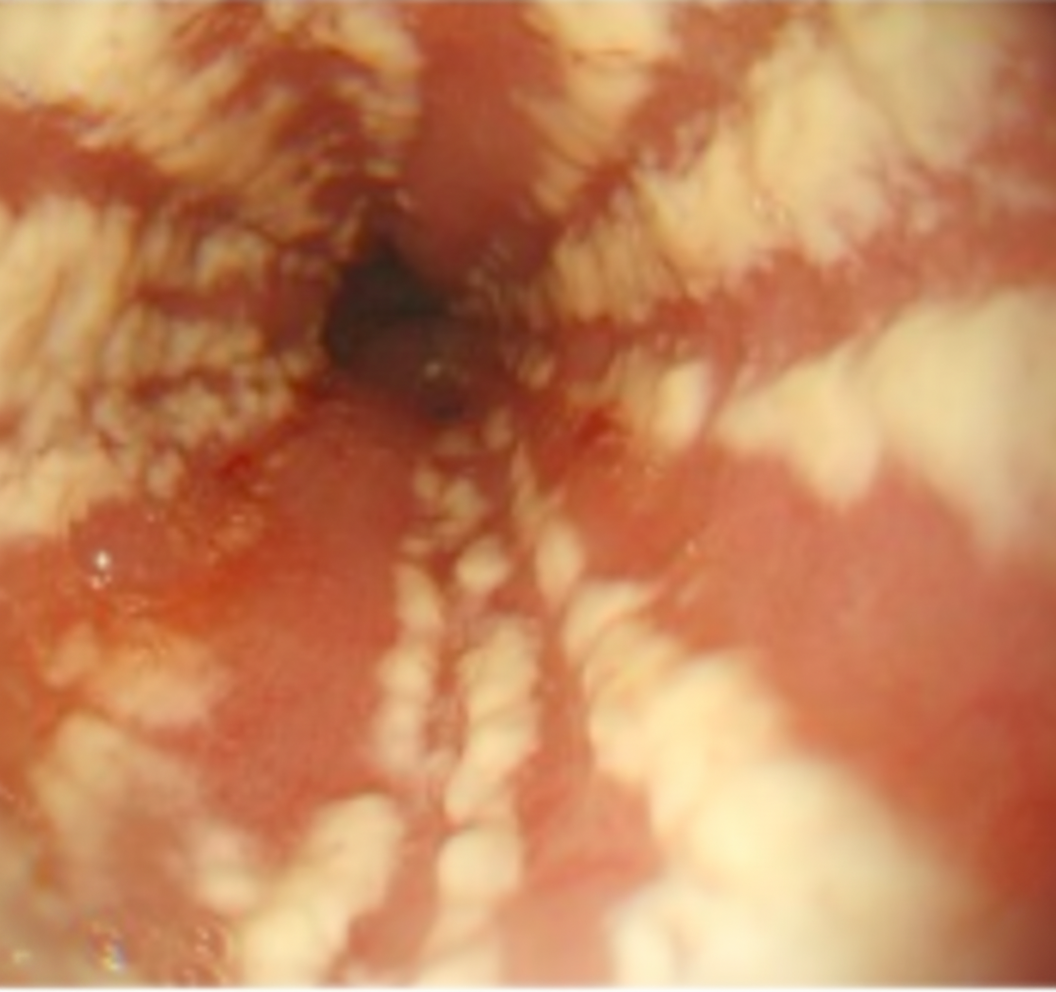
What is the drug of choice for the condition shown in the endoscopic view?
Secondary pulmonary tuberculosis usually involves which part of the lungs?
A previously healthy 43-year-old man presents with symptoms of cough, fever, weight loss, and lymphadenopathy for the past 2 months. His physical examination reveals multiple axillary and cervical lymph nodes and oropharyngeal ulcerations. His CXR reveals fibronodular pulmonary infiltrates in the apex, his sputum is negative for TB, and the HIV test is negative. A bronchoalveolar lavage (BAL) confirms the diagnosis. For the above patient, select the most likely diagnosis?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app