
Infectious Diseases — MCQs

On this page
Which of the following parasitic infestations is most commonly associated with malabsorption?
A primigravida in the first trimester was observed to be sputum positive for acid-fast bacilli, with no previous history of tuberculosis. Which treatment strategy should be employed?
Which of the following is not seen in tubercular meningitis:
In humans, cryptosporidiosis typically presents as?
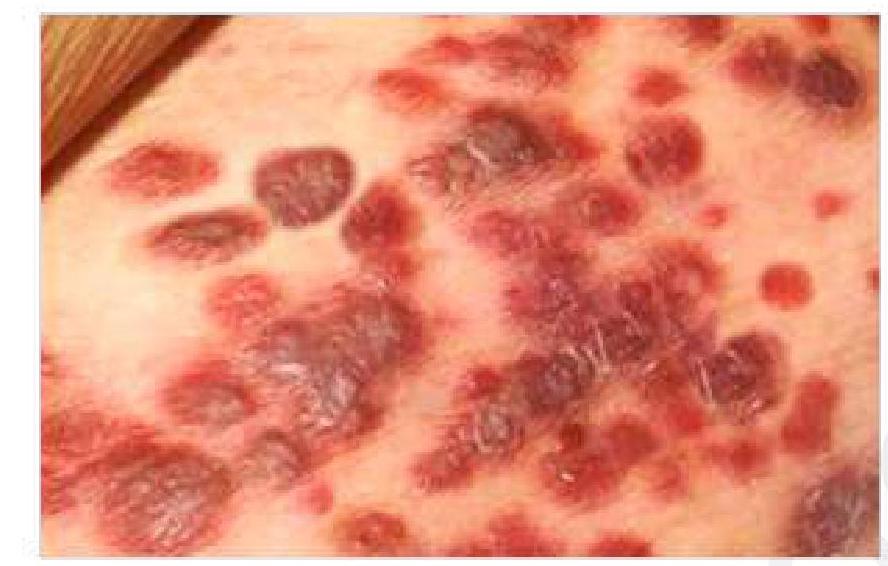
A 50-year-old HIV-positive patient presents with a painless, purple lesion on the skin. What is the most likely diagnosis?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app