
Infectious Diseases — MCQs

On this page
What is the immediate treatment of choice for severe hypotension in Dengue shock syndrome?
A male patient is HBsAg positive, HBeAg negative, and anti-HBe antibody positive. HBV DNA copies are 100,000/mL, and SGOT and SGPT are elevated to 6 times the upper limit of normal. What is the likely diagnosis?
What is the recommended duration of Miltefosine treatment for kala azar?
A patient presents with fever for 5 days, altered sensorium, increased JVP, maculopapular rash, and erythema on the back with black necrotic tissue. What is the appropriate initial treatment?
A 67-year-old man presents with persistent shooting pains, lower limb ataxia, and bladder dysfunction. Physical examination reveals small, irregular pupils that constrict with accommodation but not in response to light. A VDRL test is positive. A CT scan of the spinal cord would most likely demonstrate atrophy of which of the following structures?
A 26-year-old woman presents with a 5-day history of fever. On physical examination, her temperature is 38.2°C, pulse is 100/min, respirations are 19/min, and blood pressure is 90/60 mm Hg. A cardiac murmur is heard on auscultation. Her sensorium is clouded, but there are no focal neurologic deficits. Laboratory findings include hemoglobin, 13.1 g/dL; platelet count, 233,300/mm³; and WBC count, 19,200/mm³. Blood cultures are positive for gram-positive bacteria. Urinalysis shows hematuria. An echocardiogram reveals 1.5-cm vegetation on the mitral valve. Which of the following complications is this patient most likely to develop?
What is the drug of choice for cerebral malaria?
Which statement is FALSE regarding Tuberculosis in an HIV-positive individual?
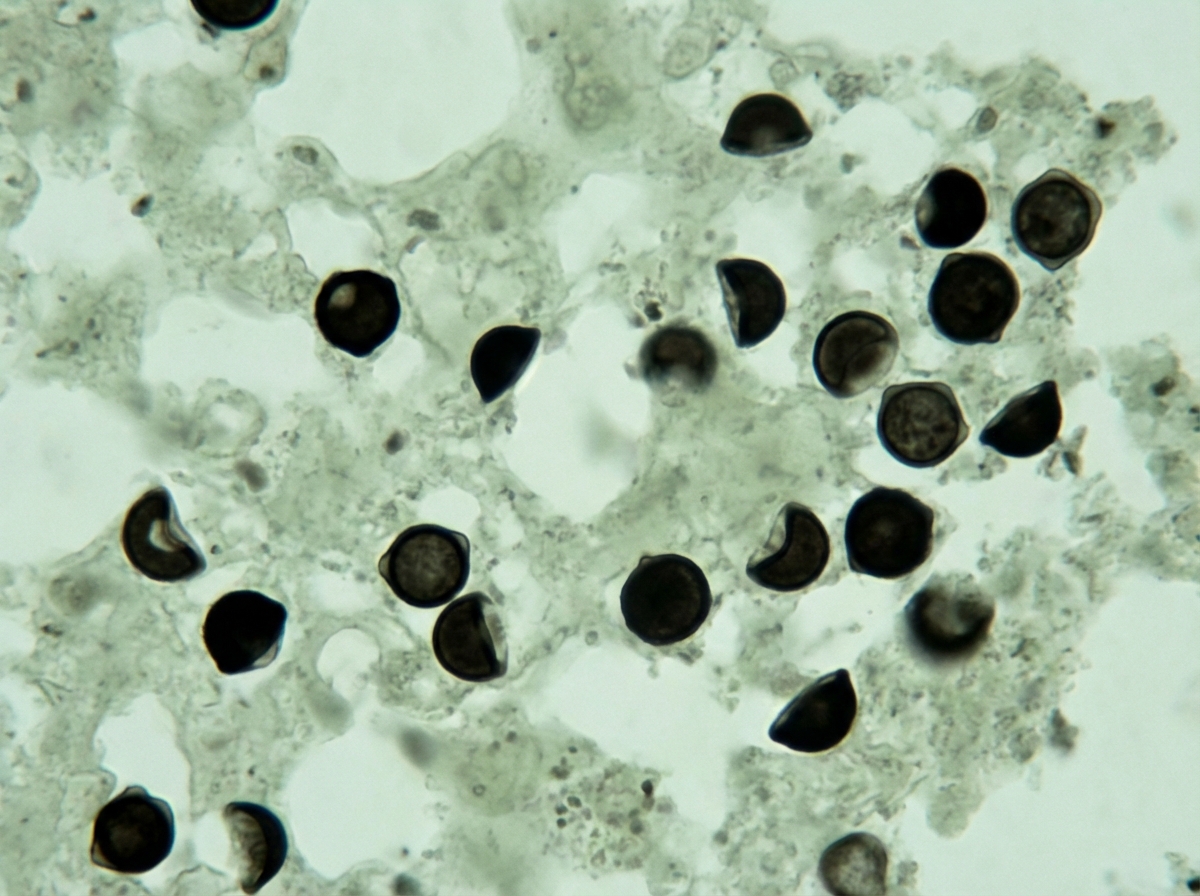
A patient with HIV and a CD4 count of 160 cells/µL presents with fever, cough, and shortness of breath for 3 weeks. Silver staining of bronchoalveolar lavage is shown. What is the drug of choice for the causative organism?
Leukopenia is characteristic of which of the following conditions?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app