
Infectious Diseases — MCQs

On this page
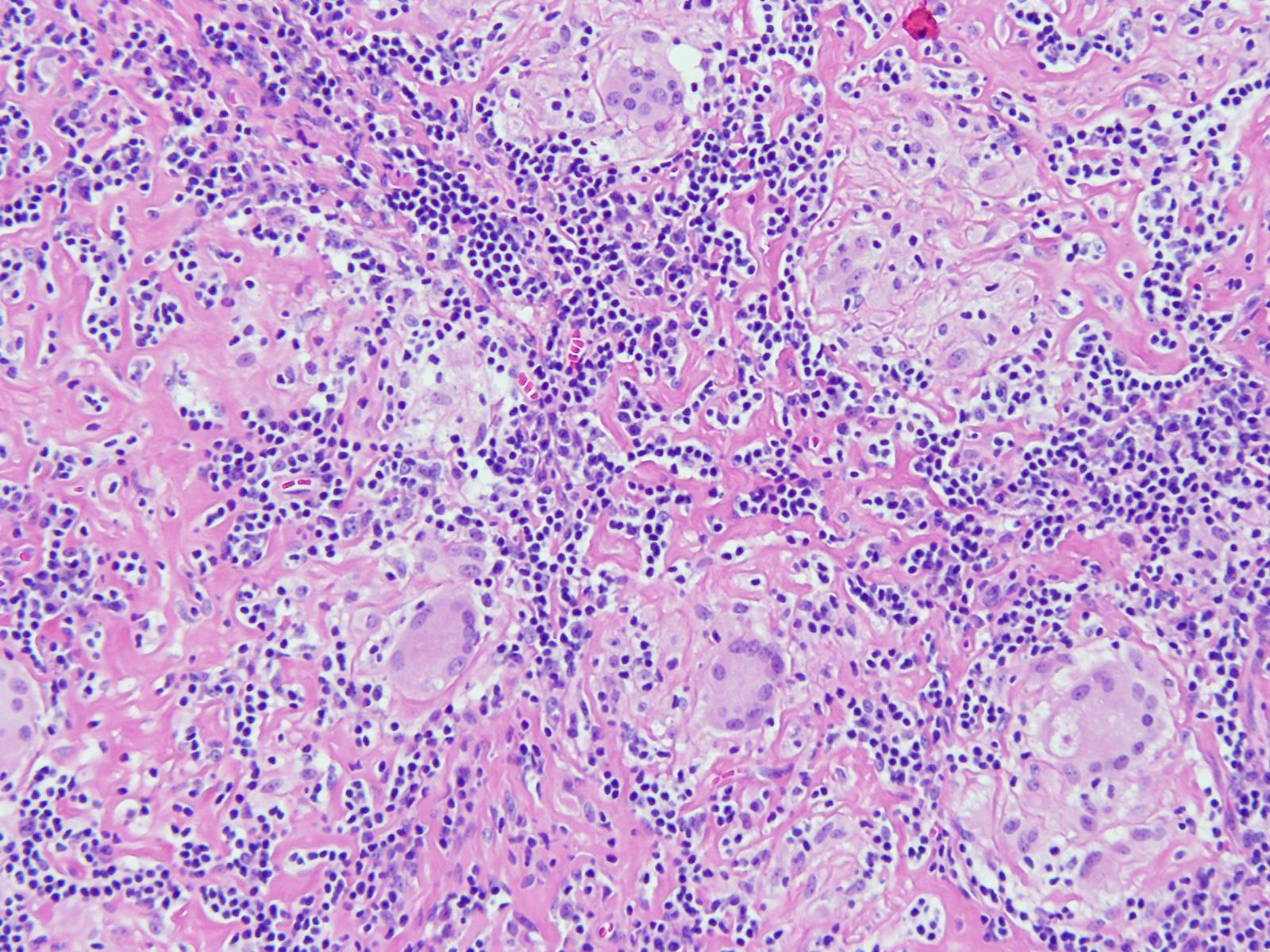
An 11-year-old boy presented with a cough for 15 days. On examination, he was found to have cervical lymphadenopathy. Lymph node biopsy showed the following findings. What could be the diagnosis?
After 4 months of renal transplantation, which infection is most likely to develop?
Which of the following conditions is least associated with HIV infection?
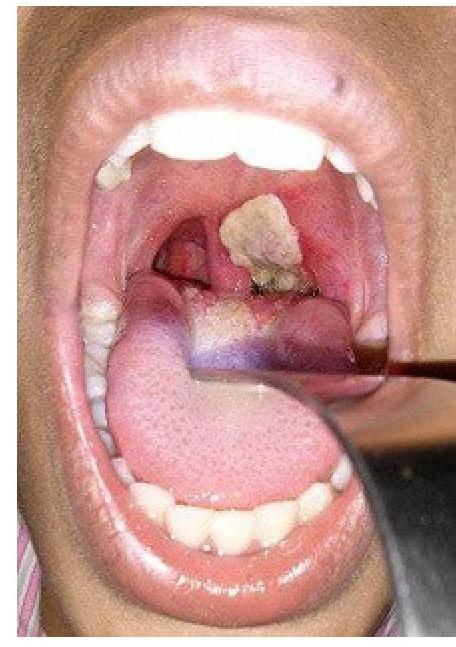
A patient presents with hoarseness of voice and a clinical condition as shown in the image. Identify the lesion:
A patient complains about painful blisters around the angle of mouth, identify the pathogen
What are the essential major blood culture criteria for diagnosing infective endocarditis?
Which virus is typically associated with serpiginous ulcers in the distal esophagus?
Pneumocystis jirovecii, typically seen in immunocompromised patients, is a:
A boy presented with multiple non suppurative osteomyelitis with sickle cell anaemia. What will be the causative organism?
What is the most commonly recommended COMPLETE antiretroviral regimen for a pregnant woman with HIV infection?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app