
Hematology — MCQs

On this page
Which of the following is NOT part of the ABVD regimen for chemotherapeutic treatment of Non-Hodgkin's Lymphoma?
What is the recommended daily amount of elemental iron required for iron replacement therapy?
While managing a febrile neutropenic patient, all of the following are essential EXCEPT:
Which of the following statements is true regarding oral therapy for iron deficiency anemia?
All of the following statements about hereditary hemochromatosis are true EXCEPT?
A patient with rheumatic heart disease, mitral stenosis, and atrial fibrillation is on oral warfarin. On an OPD visit, his INR is found to be 6. What is the recommended action?
Which of the following is a major criterion for the diagnosis of polycythemia vera?
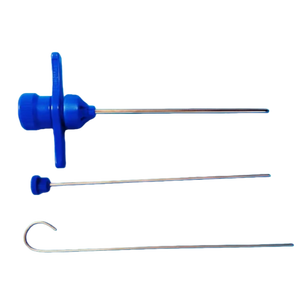
For which procedure is the following instrument used?
Which of the following is absent in hemolytic anemia?
A 28-year-old man presents with a new onset rash on both legs for 1 week. He has no past medical history and is not taking any medications. He denies recent fever but reports occasional gum bleeding and one episode of epistaxis 4 days ago. He is a non-smoker, drinks alcohol socially, and denies recreational drug use. Physical examination reveals no lymphadenopathy or hepatosplenomegaly. Laboratory studies show hemoglobin 14.8 gm/dL, hematocrit 42%, MCV 86 fL, leukocyte count 6,000/mL, and platelet count 22,000/mL. Liver and renal function tests are normal. Peripheral smear shows decreased platelet count with no red cell abnormalities. What is the most probable diagnosis?
Practice by Chapter
Anemia Evaluation and Management
Practice Questions
Hemoglobinopathies
Practice Questions
Thalassemias
Practice Questions
Platelet Disorders
Practice Questions
Coagulation Disorders
Practice Questions
Thrombotic Disorders
Practice Questions
Leukemias
Practice Questions
Lymphomas
Practice Questions
Multiple Myeloma and Plasma Cell Disorders
Practice Questions
Myeloproliferative Neoplasms
Practice Questions
Transfusion Medicine
Practice Questions
Hematopoietic Stem Cell Transplantation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app