
Clinical Manifestations and Presentation of Diseases — MCQs

On this page
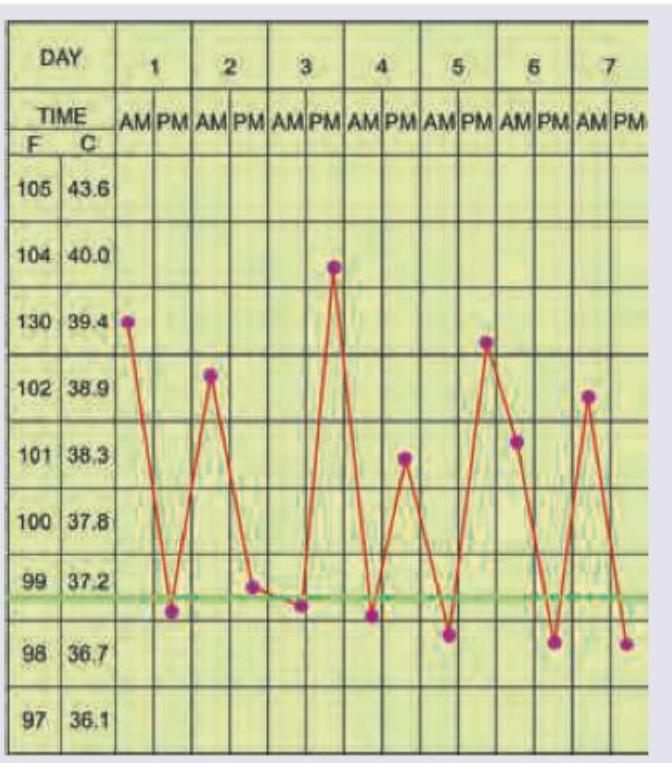
What type of fever is a patient with the following temperature charting having?
A patient presents with diffuse skin hyperpigmentation of the distal phalanges and longitudinal melanonychia with periungual hyperpigmentation. All of the following are possible diagnoses except:

In a very tall patient with arm span > height, the thumb projects beyond palm when flexed. This sign is known as:

The image shows presence of:

All are true about the clinical sign elicited except:
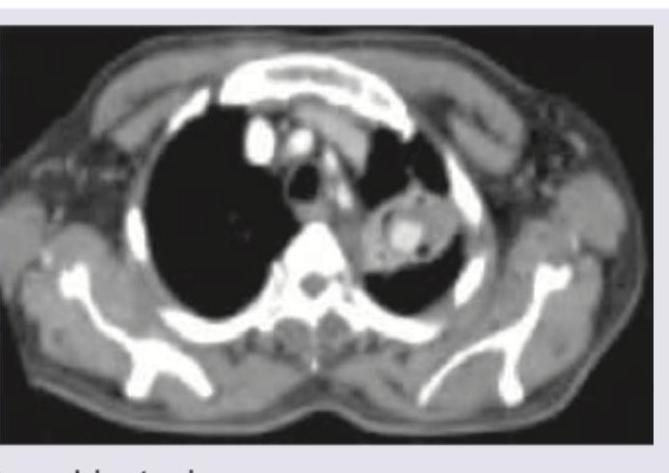
A 43-year-old diabetic male presents with cough, fever, weight loss, with loss of appetite since 2 months. CT scan shows:
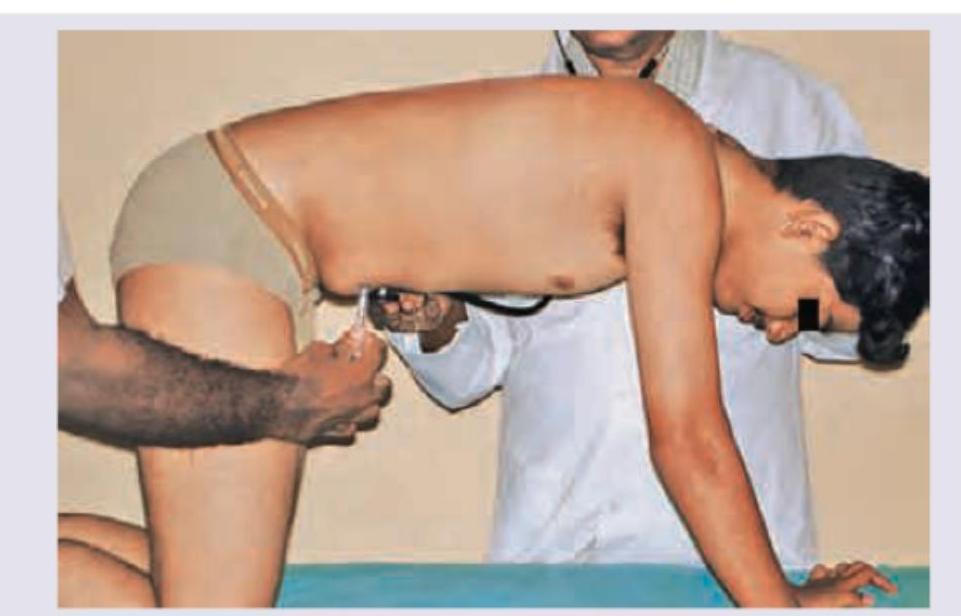
Which of the following statements is correct about the test being performed on the patient? (AIIMS May 2016)

Which of the following are considered aetiological factors for Adenocarcinoma oesophagus? I. Barrett's oesophagus II. Gastro-oesophageal reflux III. Obesity IV. Alcohol intake Select the correct answer using the code given below :
Which one of the following statements is correct for subcutaneous nodules in Rheumatic fever?
Which one of the following is a cause of exudative ascites ?
Practice by Chapter
Approach to Common Symptoms (Fever, Pain, Fatigue)
Practice Questions
Constitutional Symptoms and Their Differential Diagnosis
Practice Questions
Syncope and Presyncope
Practice Questions
Dizziness and Vertigo
Practice Questions
Dyspnea and Respiratory Distress
Practice Questions
Chest Pain Evaluation
Practice Questions
Abdominal Pain Assessment
Practice Questions
Headache Classification and Management
Practice Questions
Weight Loss and Cachexia
Practice Questions
Edema and Fluid Retention
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app