
Clinical Manifestations and Presentation of Diseases — MCQs

On this page
Which ECG finding is characteristic of hypokalemia?
Postural hypotension is not seen in which of the following conditions?
Which of the following pulmonary symptoms does NOT have a corresponding non-pulmonary association?
A patient presented with neuropsychiatric manifestations along with hepatic dysfunction. Ocular examination revealed characteristic findings. What is the initial biochemical screening test for suspected Wilson disease?

All of the following are features of Superior Vena Cava (SVC) Syndrome except?
A 60-year-old male presented to the emergency with breathlessness, facial swelling, and dilated veins on the chest wall. What is the most common cause?
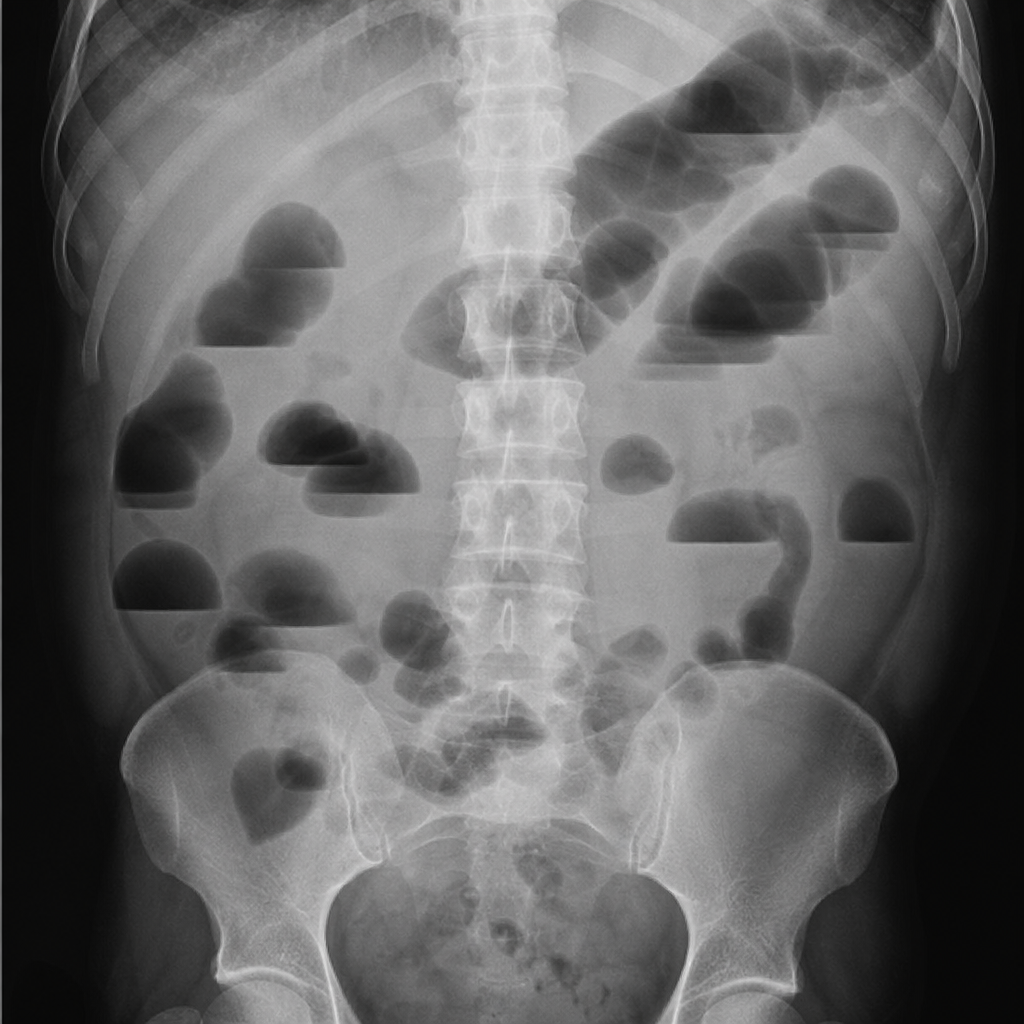
A 35-year-old male factory worker presents with severe colicky abdominal pain, constipation, and irritability for the past 2 weeks. He works in a battery recycling plant without adequate protective equipment. On examination, he has a blue-black discoloration along his gum line. CBC shows microcytic anemia, and peripheral blood smear reveals coarse basophilic stippling of red blood cells. Wrist drop is noted on neurological examination. What is the diagnosis in this patient with abdominal pain?
A patient presents with limb pain and arthralgia. The following image shows the hands, and a radiograph of the long bones reveals periosteal new bone formation along the distal extremities. The findings shown are:

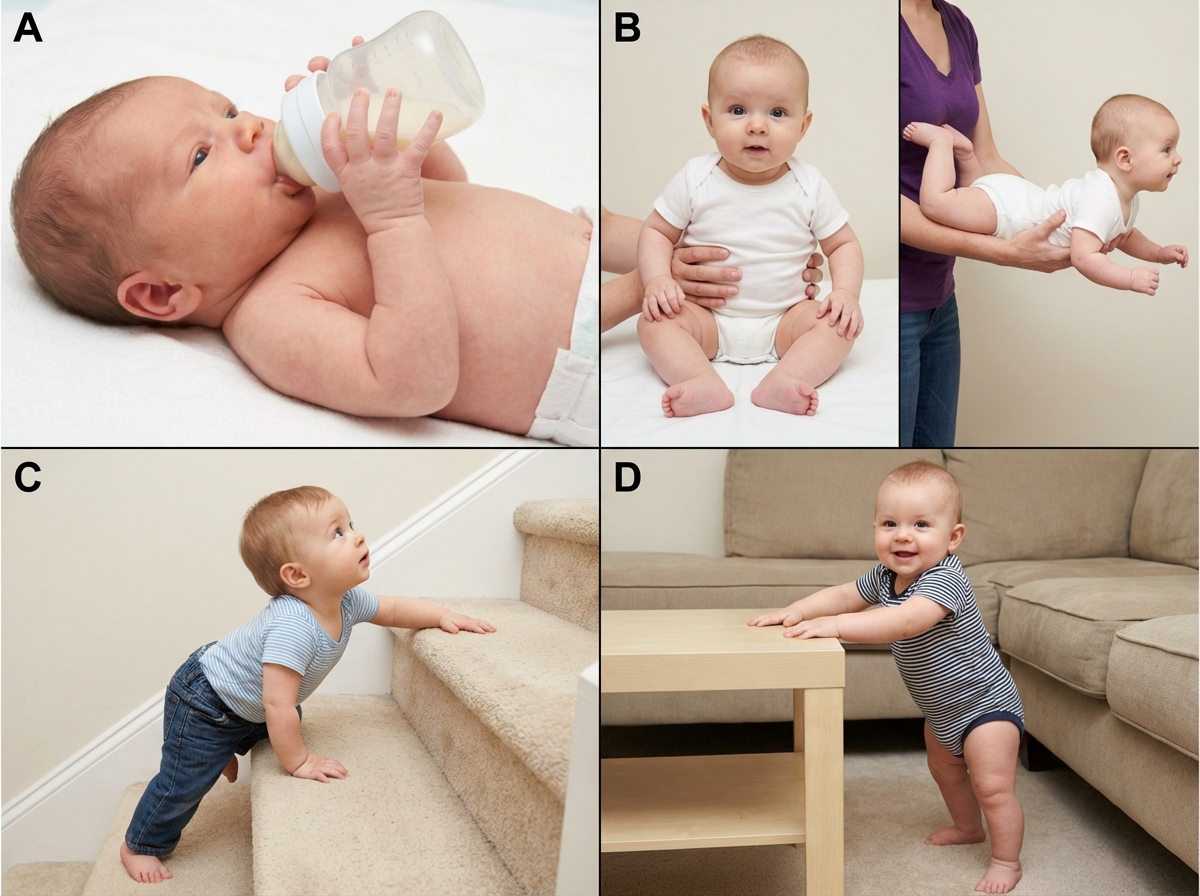
Arrange the following milestones in correct order.
An examiner is performing a deep tendon reflex examination as shown in the image. What error in technique is being demonstrated?

Practice by Chapter
Approach to Common Symptoms (Fever, Pain, Fatigue)
Practice Questions
Constitutional Symptoms and Their Differential Diagnosis
Practice Questions
Syncope and Presyncope
Practice Questions
Dizziness and Vertigo
Practice Questions
Dyspnea and Respiratory Distress
Practice Questions
Chest Pain Evaluation
Practice Questions
Abdominal Pain Assessment
Practice Questions
Headache Classification and Management
Practice Questions
Weight Loss and Cachexia
Practice Questions
Edema and Fluid Retention
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app