
Cardiology — MCQs

On this page
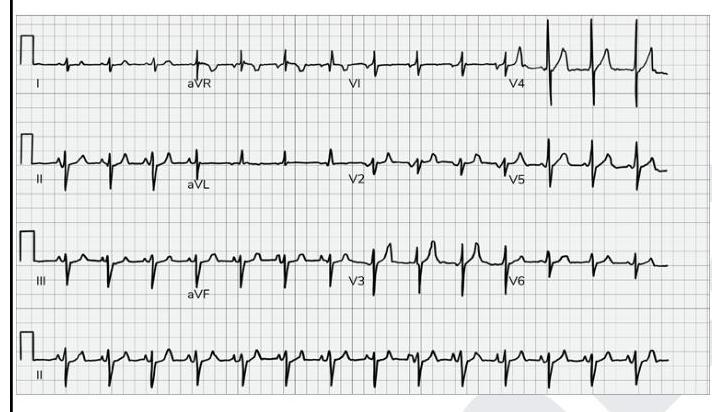
What does the given ECG show?
A 62-year-old patient presents with pain in the calf muscles while walking. The pain subsides with rest. Which of the following is not typically seen in intermittent claudication?
A 60-year-old male patient with critical mitral stenosis presented with atrial fibrillation. He has a history of multiple episodes of transient ischemic attacks. Which of the following are true regarding preventing stroke in this patient? 1. Only aspirin is given 2. Warfarin is given 3. Direct oral anticoagulants are not indicated 4. Mitral valvotomy should be recommended
A 47-year-old man comes to the physician for a follow-up examination. He feels well. He was diagnosed with hypertension 3 months ago. He has smoked one pack of cigarettes daily for 20 years but quit 4 years ago. He occasionally drinks alcohol on the weekends. He walks for 45 minutes daily and eats three meals per day. His current diet consists mostly of canned tuna and cured meats. He started eating whole-wheat bread after he was diagnosed with hypertension. He drinks 1 to 2 cups of coffee daily. His mother has a history of hyperthyroidism. Current medications include hydrochlorothiazide and a multivitamin pill every night before sleeping. His wife told him that he sometimes snores at night, but he reports that he usually sleeps well and feels refreshed in the mornings. His pulse is 80/min, respirations are 18/min, and blood pressure is 148/86 mm Hg. Physical examination shows no abnormalities. Which of the following is the most appropriate next step in the management of this patient?
A 45-year-old female with no significant past medical history present to her primary care physician for her annual check up. She missed her several appointments in the past as she says that she does not like coming to the doctor's office. When she last presented 1 year ago, she was found to have an elevated blood pressure reading. She states that she has been in her usual state of health and has no new complaints. Vital signs in the office are as follows: T 98.8 F, BP 153/95 mmHg, HR 80 bpm, RR 14 rpm, SaO2 99% on RA. She appears very anxious during the exam. The remainder of the exam is unremarkable. She reports that her blood pressure was normal when she checked it at the pharmacy 3 months ago. What test would you consider in order to further evaluate this patient?
A 58-year-old man is brought to the emergency department by his family because of severe upper back pain, which he describes as ripping. The pain started suddenly 1 hour ago while he was watching television. He has hypertension for 13 years, but he is not compliant with his medications. He denies the use of nicotine, alcohol or illicit drugs. His temperature is 36.5°C (97.7°F), the heart rate is 110/min and the blood pressure is 182/81 mm Hg in the right arm and 155/71 mm Hg in the left arm. CT scan of the chest shows an intimal flap limited to the descending aorta. Intravenous opioid analgesia is started. Which of the following is the best next step in the management of this patient condition?
A 43-year-old woman presents to her primary care provider with shortness of breath. She reports a 4-month history of progressively worsening difficulty breathing with associated occasional chest pain. She is a long-distance runner but has had trouble running recently due to her breathing difficulties. Her past medical history is notable for well-controlled hypertension for which she takes hydrochlorothiazide. She had a tibial osteosarcoma lesion with pulmonary metastases as a child and successfully underwent chemotherapy and surgical resection. She has a 10 pack-year smoking history but quit 15 years ago. She drinks a glass of wine 3 times per week. Her temperature is 98.6°F (37°C), blood pressure is 140/85 mmHg, pulse is 82/min, and respirations are 18/min. On exam, she has increased work of breathing with a normal S1 and loud P2. An echocardiogram in this patient would most likely reveal which of the following?
Raised JVP that does not fall back is a characteristic feature of which condition?
Which of the following conditions should not be considered if JVP rises on deep inspiration?
Which of the following is not a component of Jones criteria for diagnosing acute rheumatic fever?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app