
Cardiology — MCQs

On this page
The "DASH diet" is a lifestyle modification for management of which of these conditions ?
DASH diet plan is advocated in the control of which one of the following diseases?
Consider the following statements regarding claudication: 1. It is a marker for silent coronary disease 2. Structured exercise program ( 2 hours per week for 3 months) leads to improvement in symptoms 3. Diabetes mellitus increases the risk and severity of claudication 4. Beta blockers may exacerbate claudication Which of the above statements are correct?
The PR interval was measured at 0.21 seconds on a routine ECG of a patient. What is the correct interpretation?
A patient presents with shortness of breath. Vitals are HR = 120/min with BP = 90/60 mm Hg. Echocardiography shows diastolic collapse of the ventricles. What is the best management for this patient?
A 12-year-old boy presents with weak pulses in the upper limbs, a blood pressure of 90/60 mmHg , and retinal hemorrhages. What is the most likely diagnosis?
All of the following are the causes of High output cardiac failure, except?
Which of the following describes aortic regurgitation murmur?
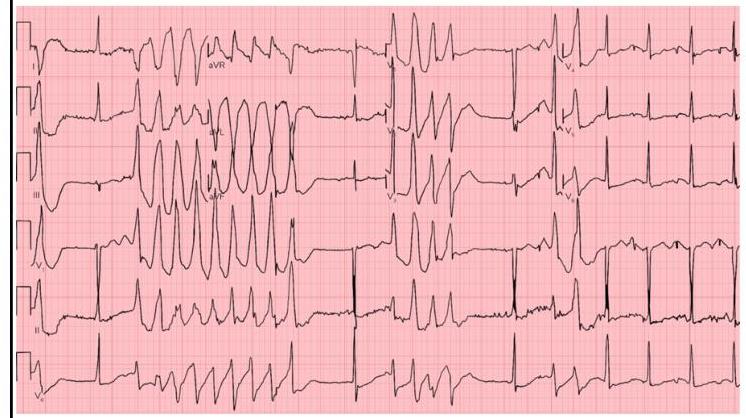
Identify the ECG given below?
What is the correct order for cardiac auscultation on the left side, from superior to inferior? a. Pulmonary b. Tricuspid c. Mitral
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app