
Cardiology — MCQs

On this page
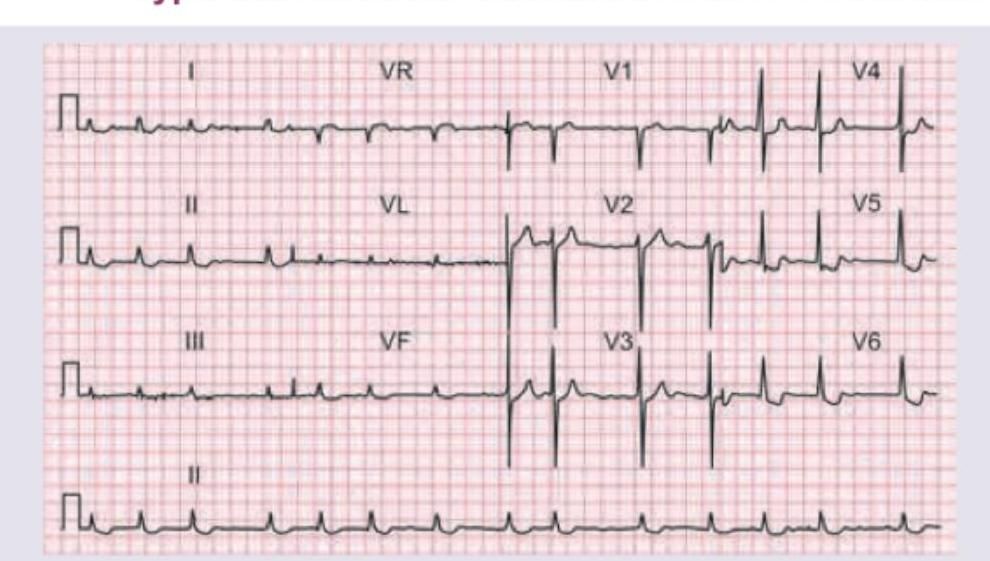
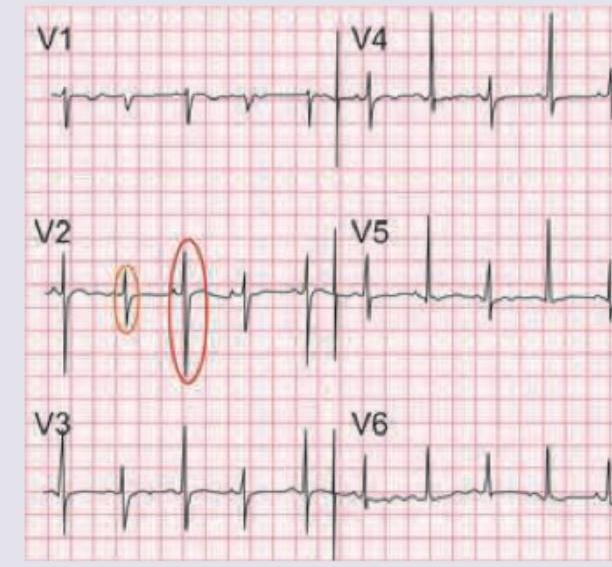
This ECG was recorded from a 60 -year-old woman with hypertension. Which is correct about the ECG shown?
This ECG is of a 23 -year-old medical student who complained of an irregular heartbeat. Other than an irregular pulse, his heart was clinically normal. What does the ECG show?
A patient presents with episodic rest chest pain due to coronary vasospasm (Prinzmetal's angina). Which of the following ECG findings will be seen during active vasospastic chest pain?
Which is correct about the ECG shown below?
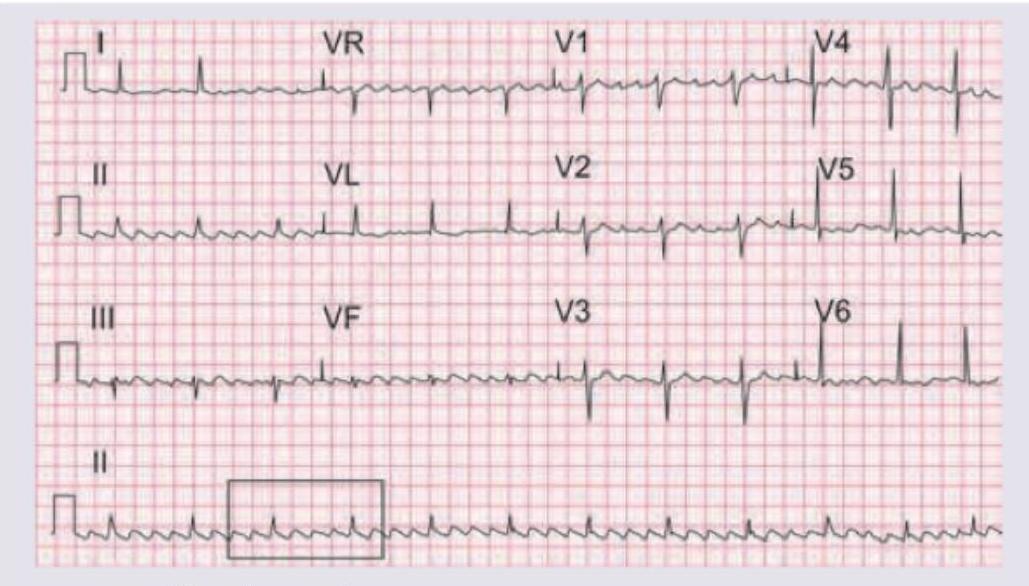
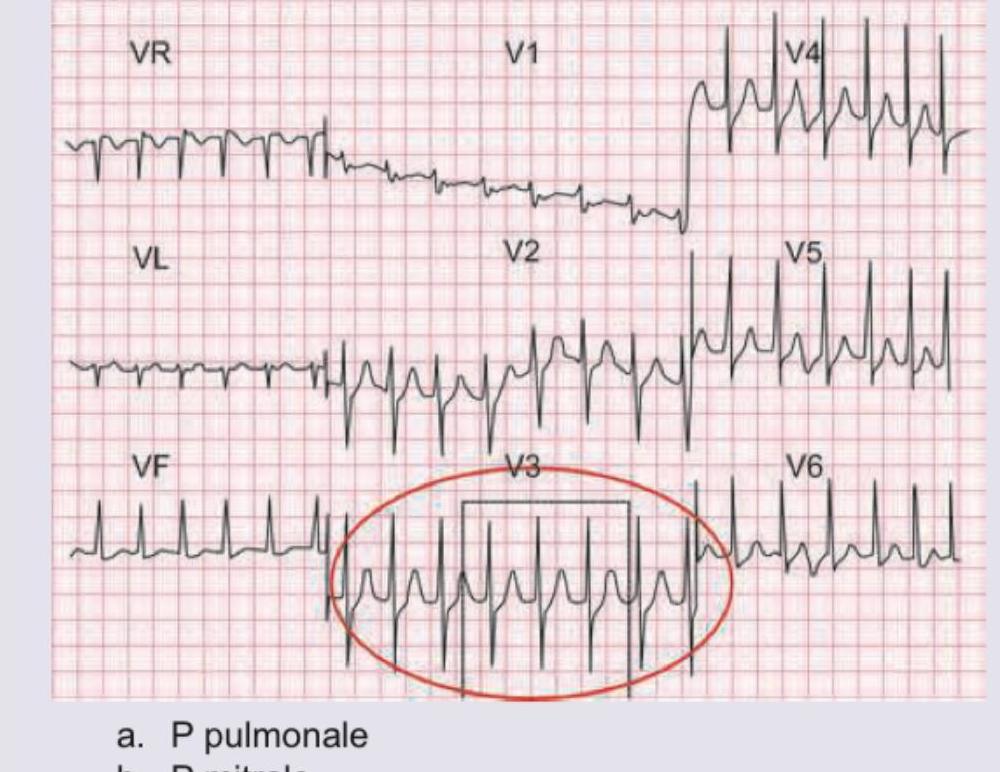
A 25-year-old girl presents with history of recurrent syncopal attacks. An ECG is obtained and shows a regular narrow-complex tachycardia at approximately 150 bpm with no clearly identifiable P waves distinct from the QRS complexes and no sawtooth flutter waves. Which is correct about the recording?
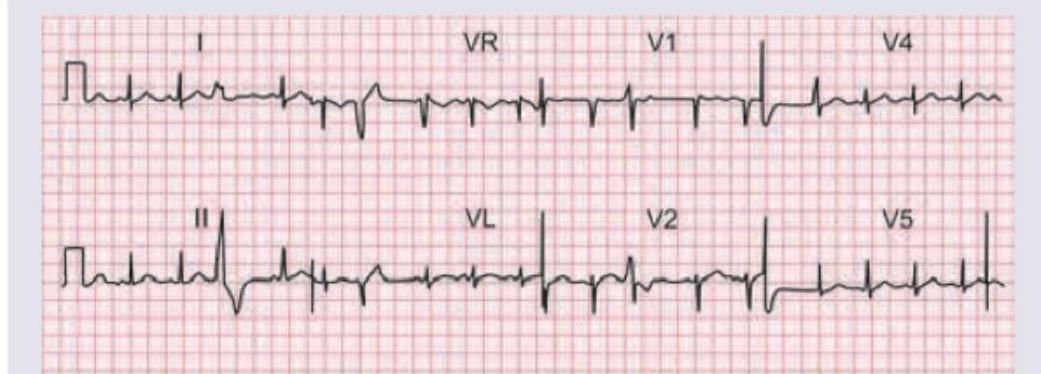
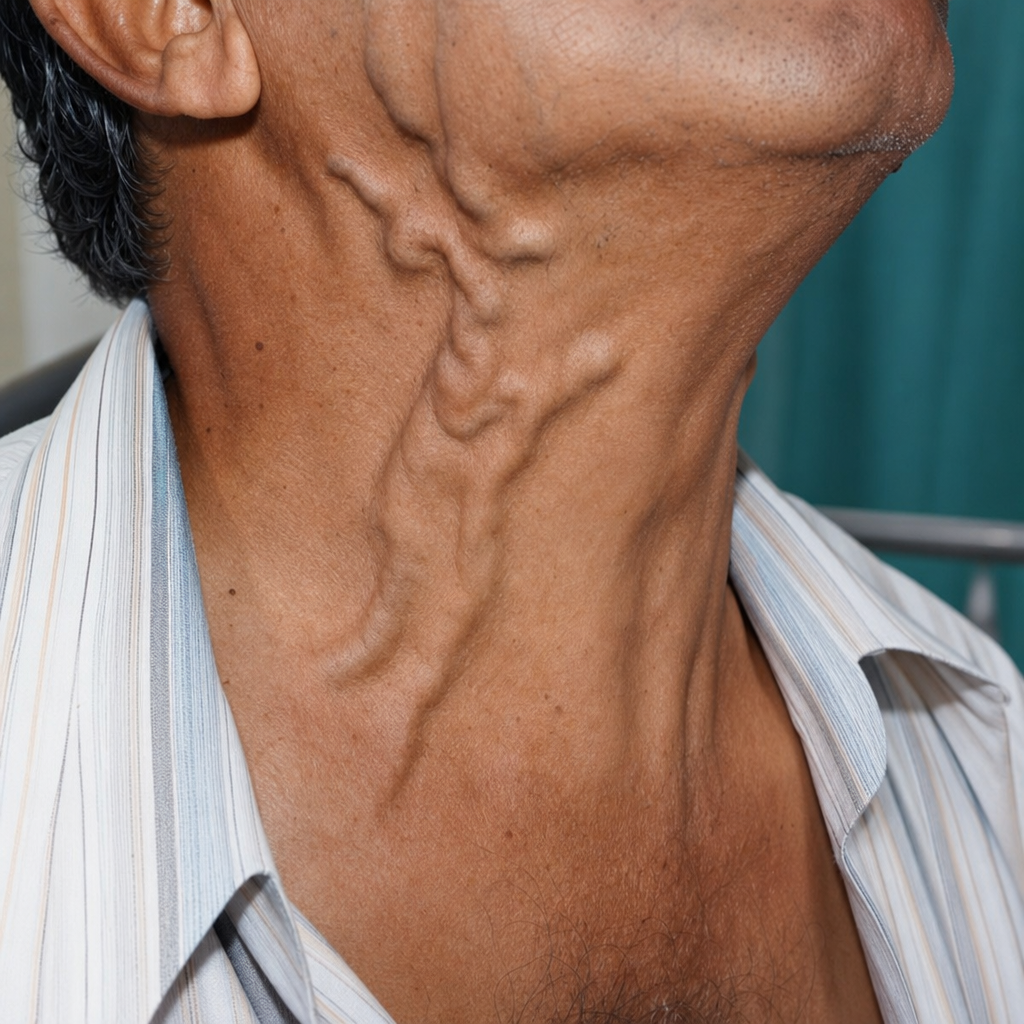
A 30-year-old male was brought to the ER after a car crash. On admission, pulse is weak with BP=80 / 60 mm Hg. ECG is shown below. Right heart catheter is placed. Which is the most consistent value with patient's diagnosis?
The murmur of mitral regurgitation is best heard at
Which of the following statements is correct regarding the Opening Snap (OS) in a patient of mitral stenosis?
Which one of the following is correct with regard to Carey Coombs murmur?
Consider the following statements for diagnosing ventricular aneurysm in a patient with recent myocardial infarction : I. Paradoxical impulse on chest wall II. Persistent ST elevation on ECG III. Unusual bulge from cardiac silhouette on X-ray IV. Presence of pulsus paradoxsus Which of the above are correct?
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app